

Does Relative Energy Deficiency in Sport (REDs) Syndrome Exist?
- PMID: 39287777
- PMCID: PMC11561064
- DOI: 10.1007/s40279-024-02108-y
Does Relative Energy Deficiency in Sport (REDs) Syndrome Exist?
Abstract
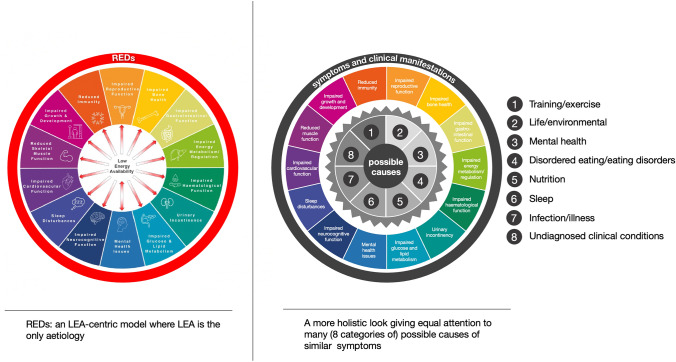
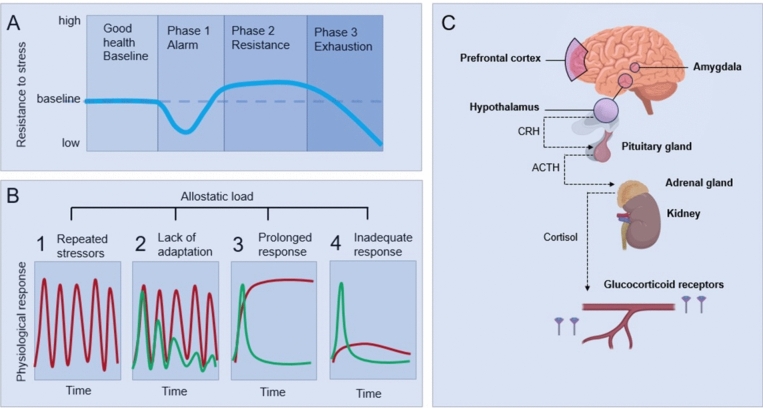
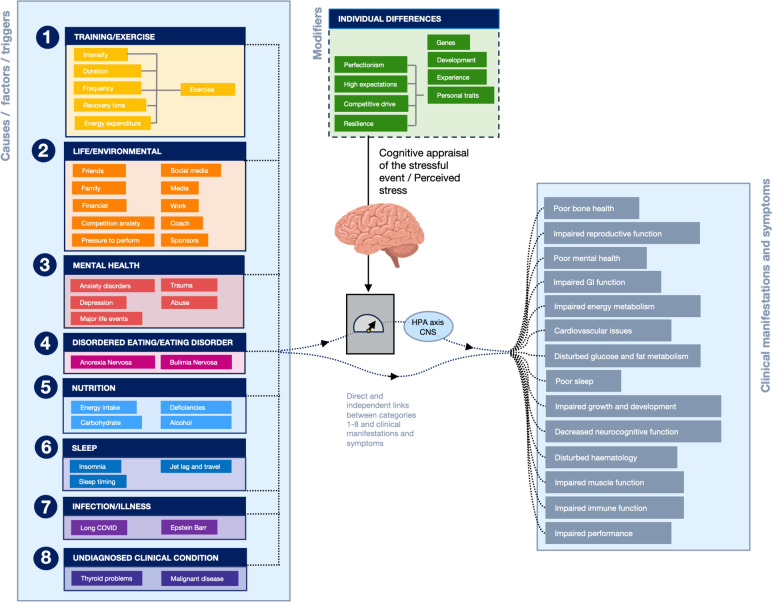
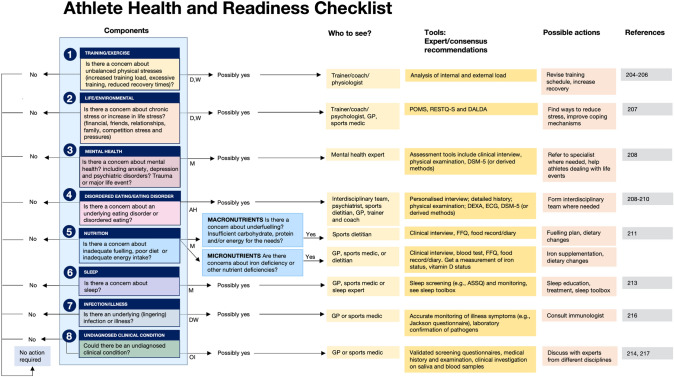
Relative energy deficiency in sport (REDs) is a widely adopted model, originally proposed by an International Olympic Committee (IOC) expert panel in 2014 and recently updated in an IOC 2023 consensus statement. The model describes how low energy availability (LEA) causes a wide range of deleterious health and performance outcomes in athletes. With increasing frequency, sports practitioners are diagnosing athletes with "REDs," or "REDs syndrome," based largely upon symptom presentation. The purpose of this review is not to "debunk" REDs but to challenge dogmas and encourage rigorous scientific processes. We critically discuss the REDs concept and existing empirical evidence available to support the model. The consensus (IOC 2023) is that energy availability, which is at the core of REDs syndrome, is impossible to measure accurately enough in the field, and therefore, the only way to diagnose an athlete with REDs appears to be by studying symptom presentation and risk factors. However, the symptoms are rather generic, and the causes likely multifactorial. Here we discuss that (1) it is very difficult to isolate the effects of LEA from other potential causes of the same symptoms (in the laboratory but even more so in the field); (2) the model is grounded in the idea that one factor causes symptoms rather than a combination of factors adding up to the etiology. For example, the model does not allow for high allostatic load (psychophysiological "wear and tear") to explain the symptoms; (3) the REDs diagnosis is by definition biased because one is trying to prove that the correct diagnosis is REDs, by excluding other potential causes (referred to as differential diagnosis, although a differential diagnosis is supposed to find the cause, not demonstrate that it is a pre-determined cause); (4) observational/cross-sectional studies have typically been short duration (< 7 days) and do not address the long term "problematic LEA," as described in the IOC 2023 consensus statement; and (5) the evidence is not as convincing as it is sometimes believed to be (i.e., many practitioners believe REDs is well established). Very few studies can demonstrate causality between LEA and symptoms, most studies demonstrate associations and there is a worrying number of (narrative) reviews on the topic, relative to original research. Here we suggest that the athlete is best served by an unbiased approach that places health at the center, leaving open all possible explanations for the presented symptoms. Practitioners could use a checklist that addresses eight categories of potential causes and involve the relevant experts if and when needed. The Athlete Health and Readiness Checklist (AHaRC) we introduce here simply consists of tools that have already been developed by various expert/consensus statements to monitor and troubleshoot aspects of athlete health and performance issues. Isolating the purported effects of LEA from the myriad of other potential causes of REDs symptoms is experimentally challenging. This renders the REDs model somewhat immune to falsification and we may never definitively answer the question, "does REDs syndrome exist?" From a practical point of view, it is not necessary to isolate LEA as a cause because all potential areas of health and performance improvement should be identified and tackled.
© 2024. The Author(s).
Conflict of interest statement
Figures
References
-
- Shanley D, Hassan A, Lunan E, Carmody S. Relative energy deficiency in sport: diagnosis and management in primary care. InnovAiT Educ Inspiration Gen Practice. 2023;16(5):229–35.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
