

CACNA1G Causes Dominantly Inherited Myoclonus-Ataxia with Intellectual Disability: A Case Report
- PMID: 39287920
- PMCID: PMC11585495
- DOI: 10.1007/s12311-024-01734-6
CACNA1G Causes Dominantly Inherited Myoclonus-Ataxia with Intellectual Disability: A Case Report
Abstract
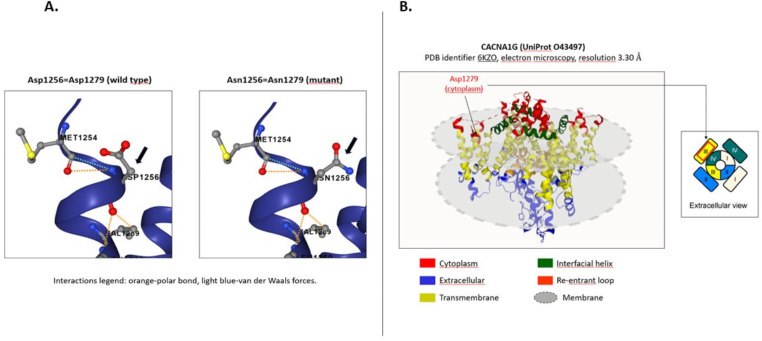
Spinocerebellar ataxias (SCAs) are characterized by substantial phenotypic variability. Among them, SCA42 is a rare non-expansion entity presenting with slowly progressive cerebellar syndrome but whose clinical spectrum may be also wider. A 53-year-old male presented with progressive myoclonus-ataxia and intellectual disability. Genetic screening revealed a novel c.3835G > A (p. Asp1279Asn) variant in the CACNA1G gene. SCA42 is a rare non-expansion SCA caused by mutations in CACNA1G on chromosome 17q21, encoding the Ca(V)3.1, a low-threshold voltage-gated T-type calcium channel. The novel variant we identified is potentially involved in channel activity. This case expands the knowledge regarding CACNA1G-associated phenotype and highlights the importance of genetic screening in myoclonus-ataxia disorders.
Keywords: CACNA1G; Ataxia; Genetic; Intellectual disability; Myoclonus.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethical Approval: The authors confirm that the approval of an institutional review board was not required for this work. A written informed consent of the patient was obtained for the publication of his data. The authors have read the Journal’s position on issues involved in the ethical publication and affirm that this work is consistent with the guidelines. Informed Consent: Patient signed informed consent regarding publishing his data and photographs. Competing Interests: The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
