Association of Vascular Risk Factors and Cerebrovascular Pathology With Alzheimer Disease Pathologic Changes in Individuals Without Dementia
- PMID: 39288341
- PMCID: PMC11450612
- DOI: 10.1212/WNL.0000000000209801
Association of Vascular Risk Factors and Cerebrovascular Pathology With Alzheimer Disease Pathologic Changes in Individuals Without Dementia
Abstract
Background and objectives: Vascular risk factors (VRFs) and cerebral small vessel disease (cSVD) are common in patients with Alzheimer disease (AD). It remains unclear whether this coexistence reflects shared risk factors or a mechanistic relationship and whether vascular and amyloid pathologies have independent or synergistic influence on subsequent AD pathophysiology in preclinical stages. We investigated links between VRFs, cSVD, and amyloid levels (Aβ1-42) and their combined effect on downstream AD biomarkers, that is, CSF hyperphosphorylated tau (P-tau181), atrophy, and cognition.
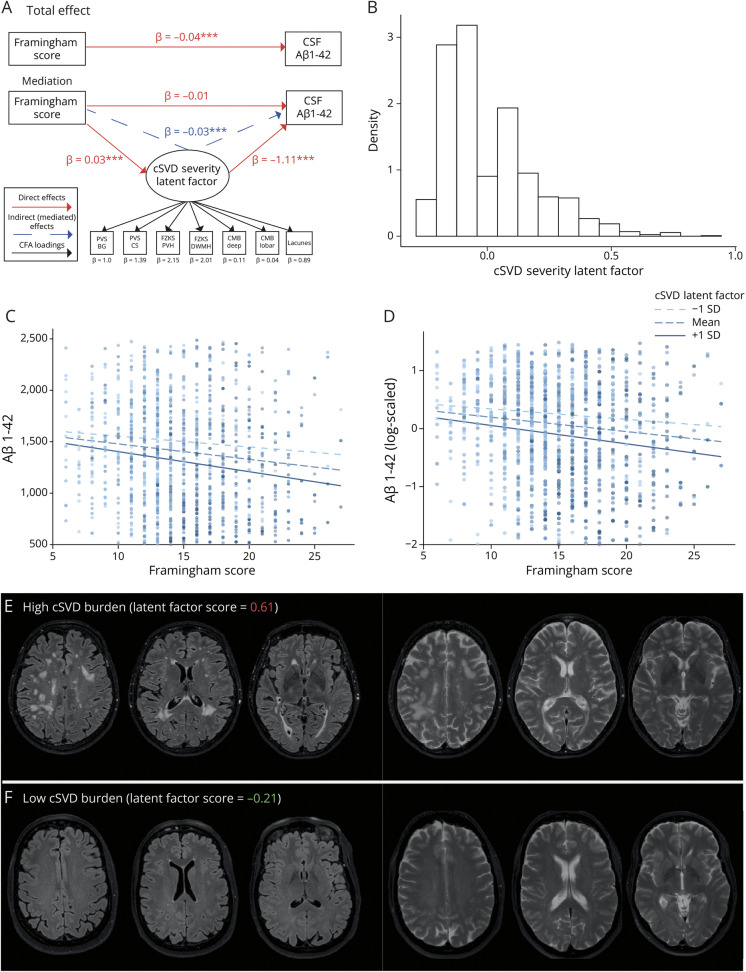
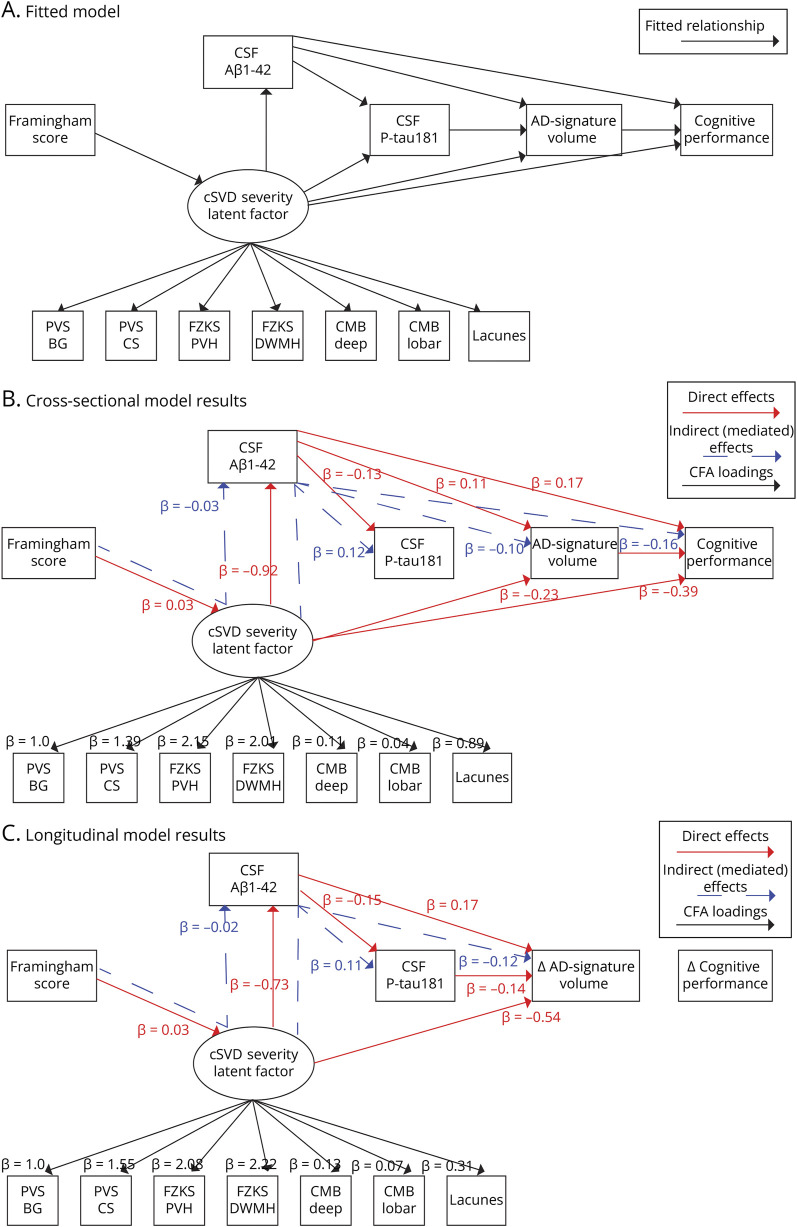
Methods: This retrospective study included nondemented participants (Clinical Dementia Rating < 1) from the European Prevention of Alzheimer's Dementia (EPAD) cohort and assessed VRFs with the Framingham risk score (FRS) and cSVD features on MRI using visual scales and white matter hyperintensity volumes. After preliminary linear analysis, we used structural equation modeling (SEM) to create a "cSVD severity" latent variable and assess the direct and indirect effects of FRS and cSVD severity on Aβ1-42, P-tau181, gray matter volume (baseline and longitudinal), and cognitive performance (baseline and longitudinal).
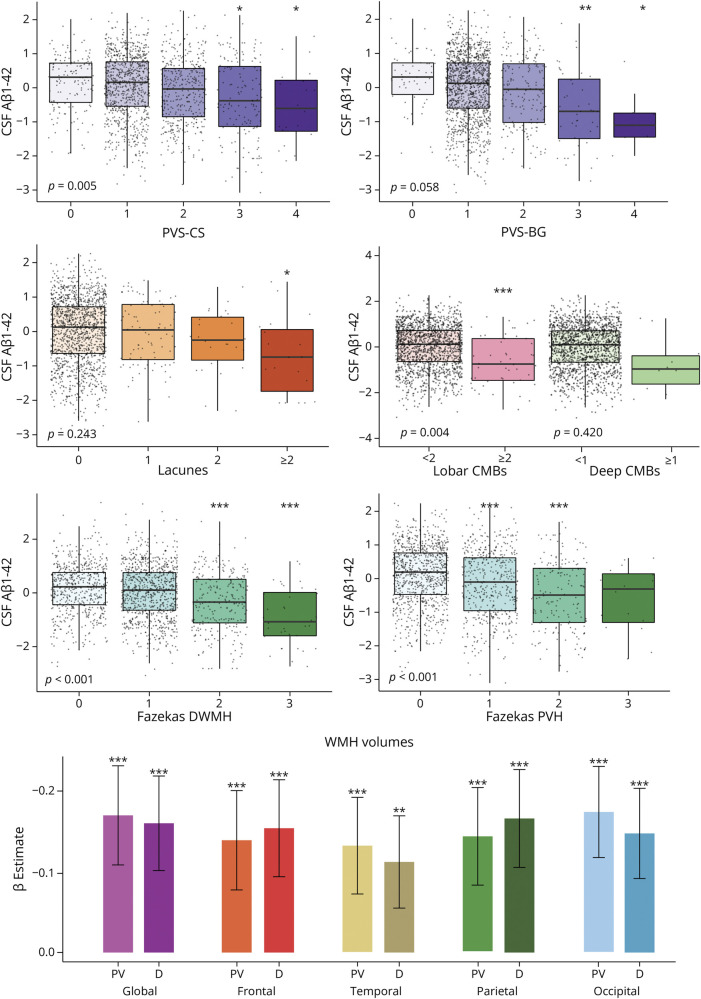
Results: A total cohort of 1,592 participants were evaluated (mean age = 65.5 ± 7.4 years; 56.16% F). We observed positive associations between FRS and all cSVD features (all p < 0.05) and a negative association between FRS and Aβ1-42 (β = -0.04 ± 0.01). All cSVD features were negatively associated with CSF Aβ1-42 (all p < 0.05). Using SEM, the cSVD severity fully mediated the association between FRS and CSF Aβ1-42 (indirect effect: β = -0.03 ± 0.01), also when omitting vascular amyloid-related markers. We observed a significant indirect effect of cSVD severity on P-tau181 (indirect effect: β = 0.12 ± 0.03), baseline and longitudinal gray matter volume (indirect effect: β = -0.10 ± 0.03; β = -0.12 ± 0.05), and baseline cognitive performance (indirect effect: β = -0.16 ± 0.03) through CSF Aβ1-42.
Discussion: In a large nondemented population, our findings suggest that cSVD is a mediator of the relationship between VRFs and CSF Aβ1-42 and affects downstream neurodegeneration and cognitive impairment. We provide evidence of VRFs indirectly affecting the pathogenesis of AD, highlighting the importance of considering cSVD burden in memory clinics for AD risk evaluation and as an early window for intervention. These results stress the role of VRFs and cerebrovascular pathology as key biomarkers for accurate design of anti-amyloid clinical trials and offer new perspectives for patient stratification.
Conflict of interest statement
L. Lorenzini, A. Maranzano and S. Ingala report no disclosures relevant to the manuscript. L.E. Collij is supported by AMYPAD (IMI 115952) and has received research support from GE HealthCare Ltd. (paid to institution). M. Tranfa, K. Blennow, and C. Di Perri report no disclosures relevant to the manuscript. C. Foley is an employee of GE HealthCare Ltd. N. C. Fox and G.B. Frisoni report no disclosures relevant to the manuscript. S. Haller is a consultant for WYSS Center, Geneva, Switzerland, and consultant for SPINEART, Geneva, Switzerland. P. Martinez-Lage and D. Mollison report no disclosures relevant to the manuscript. J. O′Brien has acted as a consultant for TauRx, Novo Nordisk, Biogen, Roche, Lilly and GE HealthCare and received grant support from Avid/Lilly, Merck and Alliance Medical. P. Payoux reports no disclosures relevant to the manuscript. C. Ritchie has done paid consultancy work in the last 3 years for Eli Lilly, Biogen, Actinogen, Brain Health Scotland, Roche, Roche Diagnostics, Novo Nordisk, Eisai, Signant, Merck, Alchemab, Sygnature and Abbvie. His group has received Research Income to his Research Unit from Biogen, AC Immune and Roche. He has out-licensed IP developed at University of Edinburgh to Linus Health and is CEO and Founder of Scottish Brain Sciences. P. Scheltens is a full-time employee of EQT Life Sciences (formerly LSP) and Professor Emeritus at Amsterdam University Medical Centers. He has received consultancy fees (paid to the university) from Alzheon, Brainstorm Cell and Green Valley. Within his university affiliation, he is global PI of the phase 1b study of AC Immune, Phase 2b study with FUJI-film/Toyama and phase 2 study of UCB. He is past chair of the EU steering committee of the phase 2b program of Vivoryon and the phase 2b study of Novartis Cardiology and presently co-chair of the phase 3 study with NOVO-Nordisk. A. J. Schwarz is an employee and minor shareholder of Takeda Pharmaceutical Company Ltd. C. H Sudre, B. M Tijms, F. Verde, N. Ticozzi report no disclosures relevant to the manuscript. V. Silani received compensation for consulting services and/or speaking activities from AveXis, Cytokinetics, Italfarmaco, Liquidweb S.r.l., Novartis Pharma AG and Zambon. Receives or has received research supports form the Italian Ministry of Health, AriSLA, E-Rare Joint Transnational Call, and the ERN Euro-NMD. He is in the Editorial Board of Amyotrophic Lateral Sclerosis and Frontotemporal Degeneration, European Neurology, American Journal of Neurodegenerative Diseases, Frontiers in Neurology, and Exploration of Neuroprotective Therapy. P. J. Visser and A. Waldman report no disclosures relevant to the manuscript. R Wolz is an employee of IXICO G. Chetalat has received research support from the European Union's Horizon 2020 research and innovation programme (grant agreement number 667696), Fondation d'entreprise MMA des Entrepreneurs du Futur, Fondation Alzheimer, Agence Nationale de la Recherche, Région Normandie, Association France Alzheimer et maladies apparentées, Fondation Vaincre Alzheimer, Fondation Recherche Alzheimer and Fondation pour la Recherche Médicale (all to Inserm) and personal fees from Inserm and Fondation Alzheimer. M. Ewers reports no disclosures relevant to the manuscript. A.M Wink is supported by AMYPAD (IMI 115952). H. Mutsaerts is supported by AMYPAD (IMI 115952) and by the Dutch Heart Foundation (2020T049), by the Eurostars-2 joint programme with co-funding from the European Union Horizon 2020 research and innovation programme (ASPIRE E!113701), provided by the Netherlands Enterprise Agency (RvO), and by the EU Joint Program for Neurodegenerative Disease Research, provided by the Netherlands Organisation for Health Research and Development and Alzheimer Nederland (DEBBIE JPND2020-568-106). J. Domingo Giaspert reports no disclosures relevant to the manuscript J. Wardlaw is supported by the UK Dementia Research Institute (funded by the MRC, Alzheimer's Society and Alzheimer's Research UK), the British Heart Foundation, the Fondation Leducq Network on Perivascular Spaces and the Row Fogo Centre for Research into Small Vessel Diseases. F. Barkhof is supported by AMYPAD (IMI 115952), EPSRC, EU-JU (IMI), NIHR-BRC, GEHC, ADDI (paid to institution), is a consultant for Combinostics, IXICO, Roche, participates in Advisory boards of USC-ATRC, Biogen, Prothena, Merck, and is a co-founder of Queen Square Analytics. Go to
Figures