

ESR Essentials: imaging of suspected child abuse-practice recommendations by the European Society of Paediatric Radiology
- PMID: 39289300
- PMCID: PMC11914366
- DOI: 10.1007/s00330-024-11052-4
ESR Essentials: imaging of suspected child abuse-practice recommendations by the European Society of Paediatric Radiology
Abstract
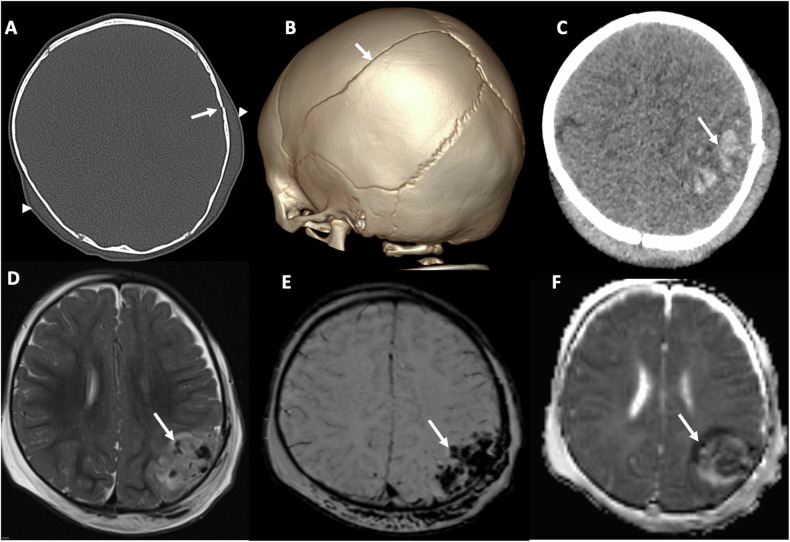
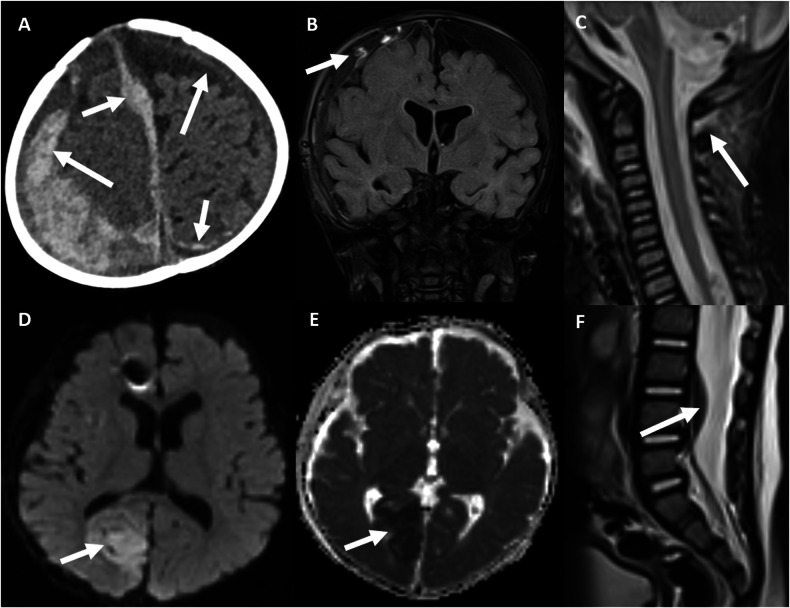
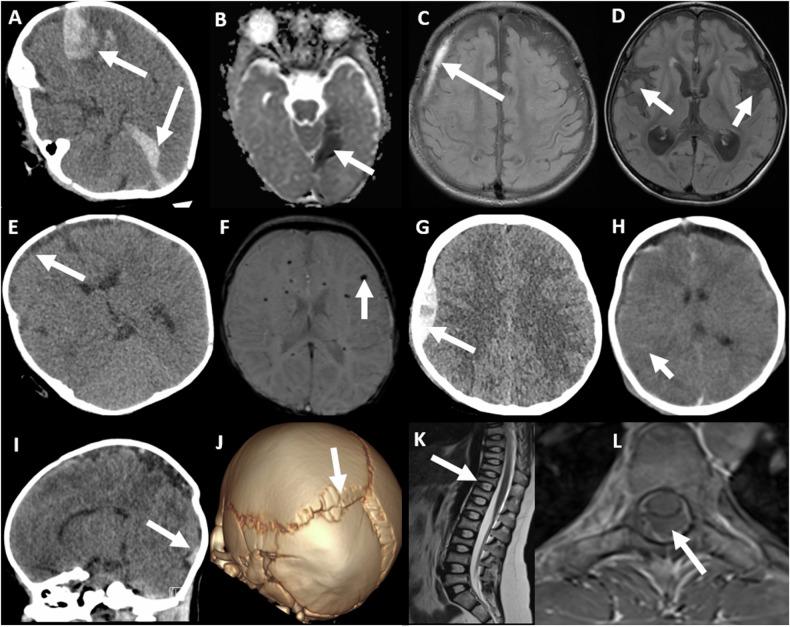
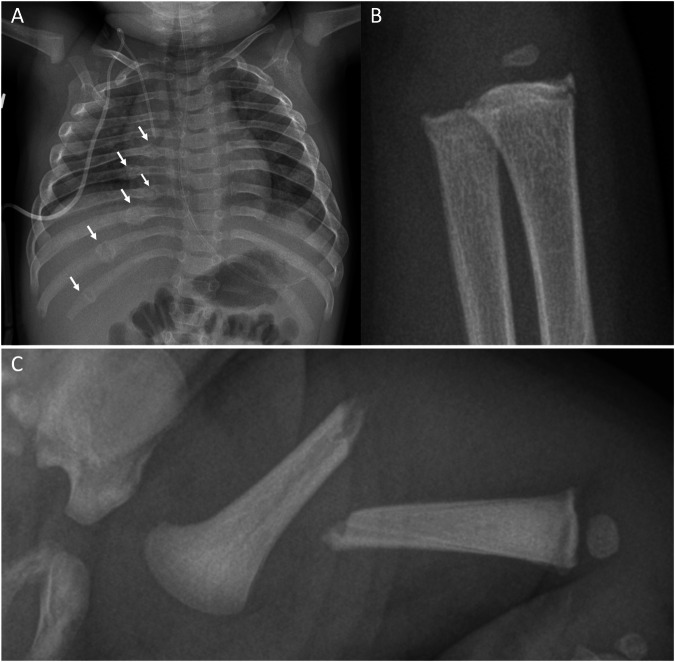
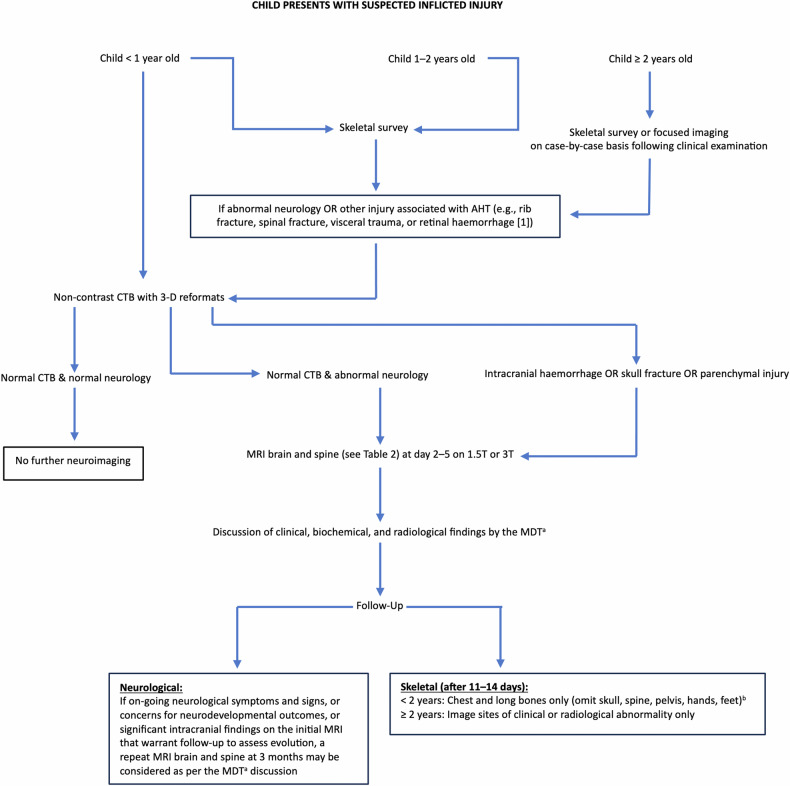
The goal of this paper is to provide a useful desktop reference for the imaging of suspected child abuse with clear, age-specific pathways for appropriate evidence-based imaging and follow-up. We aim to provide a road map for the imaging evaluation and follow-up of this important and vulnerable cohort of patients presenting with signs and symptoms concerning for inflicted injury. As the imaging recommendations differ for children of different ages, we provide a flowchart of the appropriate imaging pathway for infants, toddlers, and older children, which allows ease of selection of which children should undergo skeletal survey, non-contrast computed tomography (CT) brain with 3-dimensional (D) reformats, and magnetic resonance imaging (MRI) of the brain and whole spine. For ease of review, we include a table of the common intracranial and spinal patterns of injury in abusive head trauma. We summarise search patterns, areas of review, and key findings to include in the report. To exclude skeletal injury, infants and children under 2 years of age should undergo a full skeletal survey in accordance with national guidelines, with a limited follow-up skeletal survey performed 11-14 days later. For children over 2 years of age, the need for skeletal imaging should be decided on a case-by-case basis. All infants should undergo a non-contrast-enhanced CT brain with 3-D reformats. If this is normal with no abnormal neurology, then no further neuroimaging is required. If this is abnormal, then they should proceed to MRI brain and whole spine within 2-5 days. Children older than 1 year of age who have abnormal neurology and/or findings on skeletal survey that are suggestive of inflicted injury should undergo non-contrast CT brain with 3-D reformats and, depending on the findings, may also require MRI of the brain and whole spine. We hope that this will be a helpful contribution to the radiology literature, particularly for the general radiologist with low volumes of paediatrics in their practice, supporting them with managing these important cases when they arise in daily practice. KEY POINTS: The choice of initial imaging (skeletal survey and/or brain CT) depends on the age of the child in whom abuse is suspected. A follow-up skeletal survey is mandatory 11-14 days after the initial survey. If an MRI of the brain is performed, then an MRI of the whole spine should be performed concurrently.
Keywords: Child; Clinical protocols; Diffuse axonal injury; Fractures (bone); Physical abuse.
© 2024. The Author(s).
Conflict of interest statement
Compliance with ethical standards. Guarantor: The scientific guarantor of this publication is Amaka C. Offiah. Conflict of interest: Amaka C. Offiah: Editor of the journal Pediatric Radiology. Statistics and biometry: No complex statistical methods were necessary for this paper. Informed consent: Written informed consent was not required. Ethical approval: Institutional Review Board approval was not required. Study subjects or cohorts overlap: Not applicable. Methodology: Practice recommendations
Figures
Similar articles
-
ACR Appropriateness Criteria® Suspected Physical Abuse-Child.J Am Coll Radiol. 2017 May;14(5S):S338-S349. doi: 10.1016/j.jacr.2017.01.036. J Am Coll Radiol. 2017. PMID: 28473090 Review.
-
Whole-Spine MRI in Children With Suspected Abusive Head Trauma.AJR Am J Roentgenol. 2022 Jun;218(6):1074-1087. doi: 10.2214/AJR.21.26674. Epub 2022 Jan 12. AJR Am J Roentgenol. 2022. PMID: 35018794
-
Controversial aspects of imaging in child abuse: a second roundtable discussion from the ESPR child abuse taskforce.Pediatr Radiol. 2023 Apr;53(4):739-751. doi: 10.1007/s00247-023-05618-5. Epub 2023 Mar 7. Pediatr Radiol. 2023. PMID: 36879046 Free PMC article.
-
Vesicoureteral Reflux.2024 Apr 30. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Apr 30. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 33085409 Free Books & Documents.
-
Abusive spinal injury: imaging and updates.Pediatr Radiol. 2024 Oct;54(11):1797-1808. doi: 10.1007/s00247-024-06043-y. Epub 2024 Sep 5. Pediatr Radiol. 2024. PMID: 39235479 Free PMC article. Review.
Cited by
-
Orthodontic appliances and their diagnostic impact to brain MRI.Clin Oral Investig. 2025 Mar 22;29(4):202. doi: 10.1007/s00784-025-06275-8. Clin Oral Investig. 2025. PMID: 40119988 Free PMC article.
References
-
- Sibert JR, Payne EH, Kemp AM et al (2002) The incidence of severe physical child abuse in Wales. Child Abuse Negl 26:267–276 - PubMed
-
- Biswas A, Shroff MM (2021) Abusive head trauma: Canadian and global perspectives. Pediatr Radiol 51:876–882 - PubMed
-
- Girard N, Brunel H, Dory-Lautrec P, Chabrol B (2016) Neuroimaging differential diagnoses to abusive head trauma. Pediatr Radiol 46:603–614 - PubMed
-
- Choudhary AK, Servaes S, Slovis TL et al (2018) Consensus statement on abusive head trauma in infants and young children. Pediatr Radiol 48:1048–1065 - PubMed
-
- Biswas A, Krishnan P, Albalkhi I, Mankad K, Shroff M (2023) Imaging of abusive head trauma in children. Neuroimaging Clin N Am 33:357–373 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
