

Longitudinal deep neural networks for assessing metastatic brain cancer on a large open benchmark
- PMID: 39289405
- PMCID: PMC11408643
- DOI: 10.1038/s41467-024-52414-2
Longitudinal deep neural networks for assessing metastatic brain cancer on a large open benchmark
Abstract
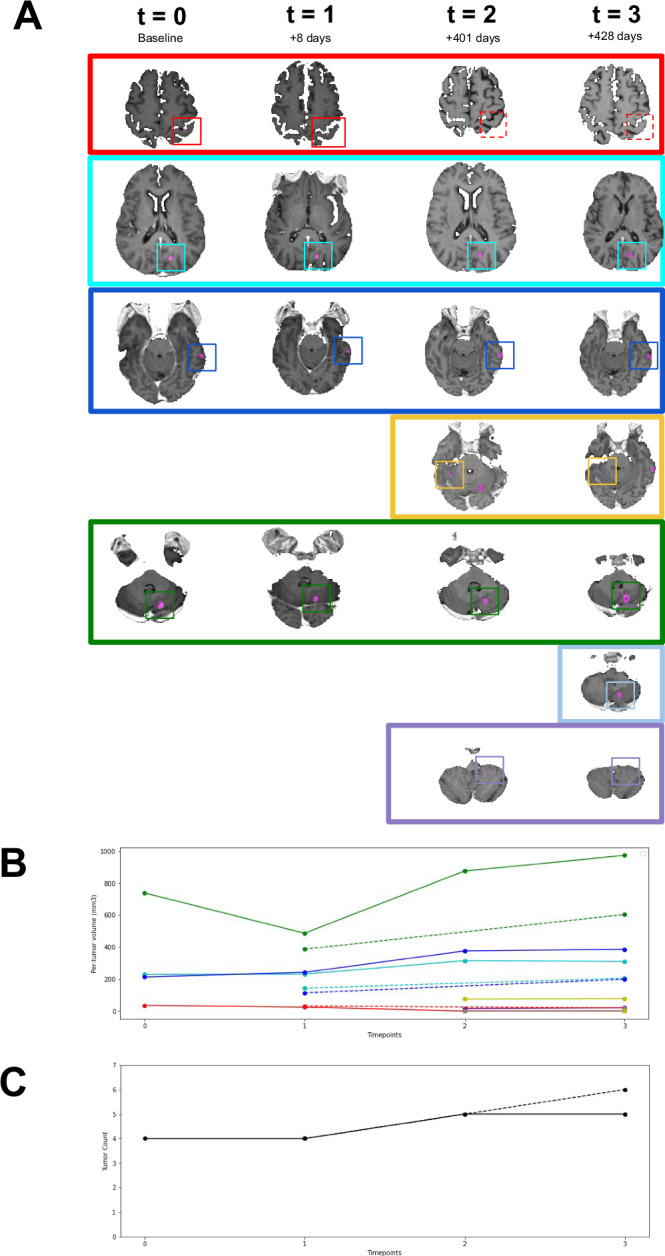
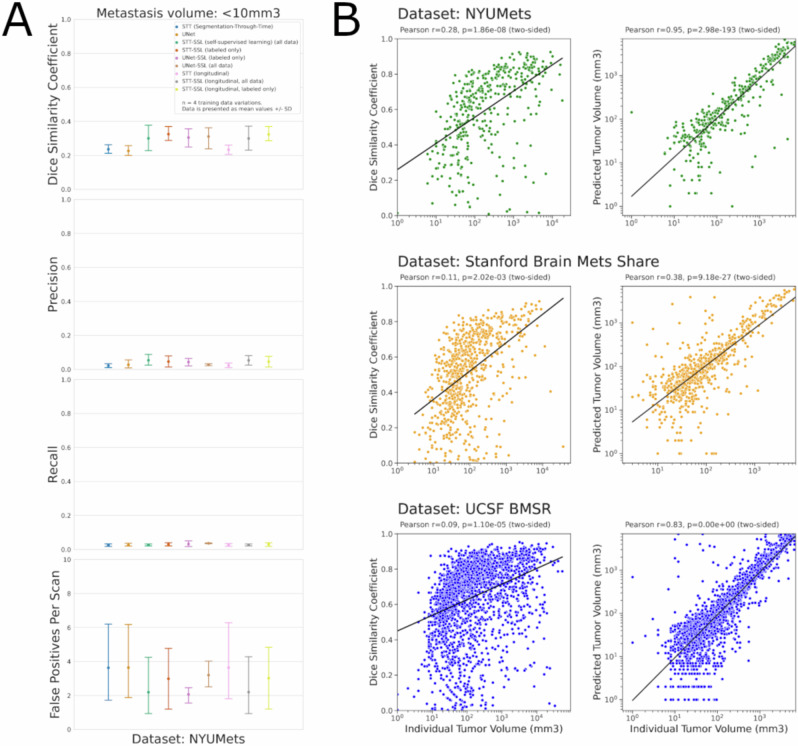
The detection and tracking of metastatic cancer over the lifetime of a patient remains a major challenge in clinical trials and real-world care. Advances in deep learning combined with massive datasets may enable the development of tools that can address this challenge. We present NYUMets-Brain, the world's largest, longitudinal, real-world dataset of cancer consisting of the imaging, clinical follow-up, and medical management of 1,429 patients. Using this dataset we developed Segmentation-Through-Time, a deep neural network which explicitly utilizes the longitudinal structure of the data and obtained state-of-the-art results at small (<10 mm3) metastases detection and segmentation. We also demonstrate that the monthly rate of change of brain metastases over time are strongly predictive of overall survival (HR 1.27, 95%CI 1.18-1.38). We are releasing the dataset, codebase, and model weights for other cancer researchers to build upon these results and to serve as a public benchmark.
© 2024. The Author(s).
Conflict of interest statement
The authors declare the following competing interests. E.K.O. reports consulting with Sofinnova Inc., Google Inc., income from Merck & Co., and Mirati Therapeutics, and equity in Artisight Inc. D.O. is a consultant and equity holder of Invenio Inc. D.K. reports consulting with Elekta Inc. K.E.L. is currently employed by NVIDIA. L.Y.J., M.N., S.N., J.D.A., K.B., T.Q., V.C., E.Y., and J.G.G. declare no competing interests. The work presented herein was performed exclusively within the NYU Langone Health System.
Figures


References
-
- Acosta, J. N., Falcone, G. J., Rajpurkar, P. & Topol, E. J. Multimodal biomedical AI. Nat. Med.28, 1773–1784 (2022). - PubMed
-
- Acosta, J. N., Falcone, G. J. & Rajpurkar, P. The need for medical artificial intelligence that incorporates prior images. Radiology10.1148/radiol.212830 (2022). - PubMed
-
- Suh, C. H., Jung, S. C., Kim, K. W. & Pyo, J. The detectability of brain metastases using contrast-enhanced spin-echo or gradient-echo images: a systematic review and meta-analysis. J. Neurooncol.129, 363–371 (2016). - PubMed
-
- Litière, S., Collette, S., de Vries, E. G. E., Seymour, L. & Bogaerts, J. RECIST - learning from the past to build the future. Nat. Rev. Clin. Oncol.14, 187–192 (2017). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
