

Exploring the relationship between live microbe intake and obesity prevalence in adults
- PMID: 39289456
- PMCID: PMC11408724
- DOI: 10.1038/s41598-024-72961-4
Exploring the relationship between live microbe intake and obesity prevalence in adults
Abstract
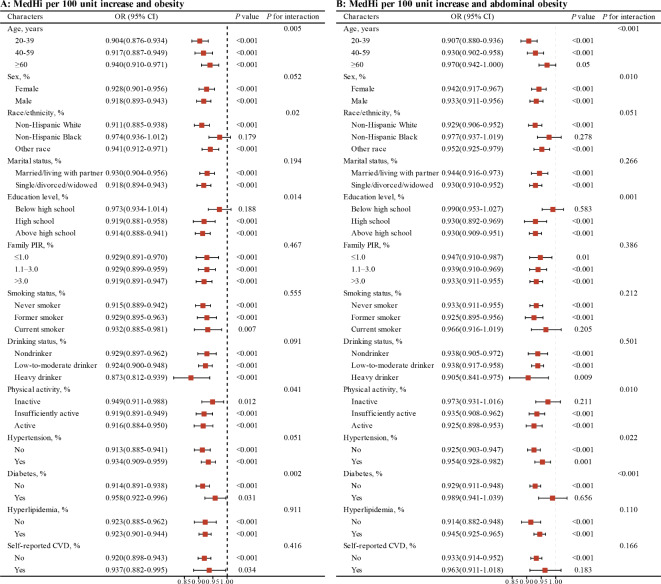
Obesity has become a global health problem. In recent years, the influence of dietary microbes in the obese population has attracted the attention of scholars. Our study aimed to investigate the link between live microbe intake and obesity in adults. Participants (aged over 20 years) for this study were from the 1999-2018 National Health and Nutrition Examination Survey (NHANES). Participants were categorised into low, medium and high dietary live microbe intake groups. Linear regression was used to analyse the link between live microbe intake and body mass index (BMI) and waist circumference (WC). Logistic regression was used to analyse the link between live microbe intake and obesity and abdominal obesity prevalence. Restricted cubic spline curves (RCS) were used to check whether there was a non-linear relationship between live microbe intake and obesity. A total of 42,749 participants were included in this study and the number of obese reached 15,463. We found that live microbe intake was negatively linked to BMI and WC. In models adjusted for all confounders, the high live microbe intake group had lower obesity (OR = 0.812, 95%CI: 0.754-0.873) and abdominal obesity prevalence (OR = 0.851, 95%CI: 0.785-0.923) than the lowest intake group. Upon further quantification of live microbe intake, we found similar results. RCS analyses showed that live microbe intake was nonlinearly negatively correlated with BMI, WC, obesity, and abdominal obesity prevalence (P for non-linearity < 0.05). This study preliminarily reveals a negative link between live microbe intake and obesity in adults.
Keywords: Abdominal obesity; Dietary live microbe; MedHi; NHANES; Obesity.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Perdomo, C. M., Cohen, R. V., Sumithran, P., Clement, K. & Fruhbeck, G. Contemporary medical, device, and surgical therapies for obesity in adults. Lancet. 401(10382), 1116–1130 (2023). - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
