

Mechanistic insights into lethal hyper progressive disease induced by PD-L1 inhibitor in metastatic urothelial carcinoma
- PMID: 39289546
- PMCID: PMC11408499
- DOI: 10.1038/s41698-024-00707-6
Mechanistic insights into lethal hyper progressive disease induced by PD-L1 inhibitor in metastatic urothelial carcinoma
Abstract
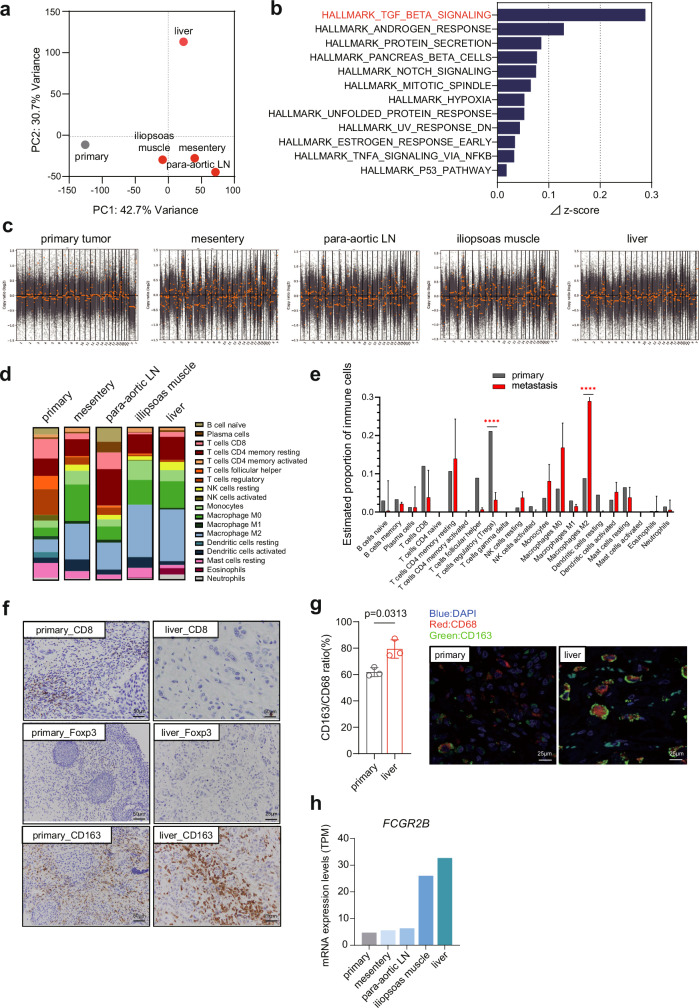
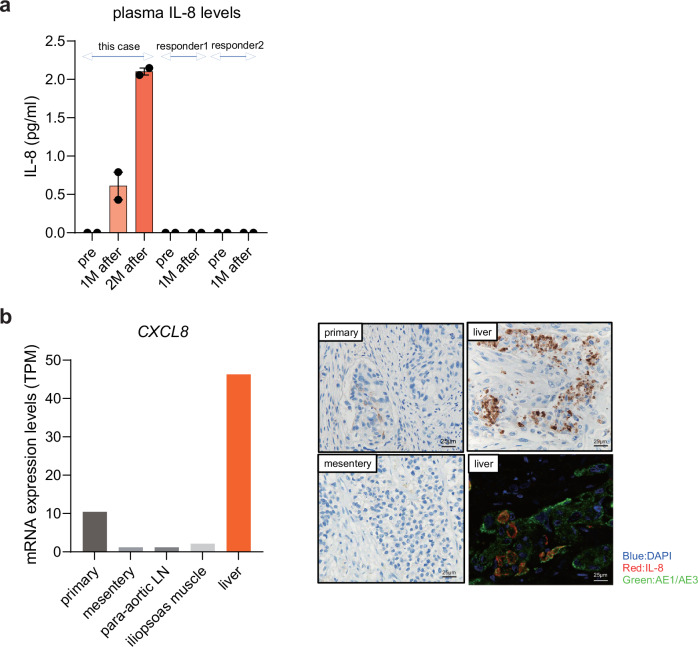
Hyper progressive disease (HPD) is a paradoxical phenomenon characterized by accelerated tumor growth following treatment with immune checkpoint inhibitors. However, the pathogenic causality and its predictor remain unknown. We herein report a fatal case of HPD in a 50-year-old man with metastatic bladder cancer. He had achieved a complete response (CR) through chemoradiation therapy followed by twelve cycles of chemotherapy, maintaining CR for 24 months. Three weeks after initiating maintenance use of a PD-L1 inhibitor, avelumab, a massive amount of metastases developed, leading to the patient's demise. Omics analysis, utilizing metastatic tissues obtained from an immediate autopsy, implied the contribution of M2 macrophages, TGF-β signaling, and interleukin-8 to HPD pathogenesis.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
