

Association of neutrophil-to-lymphocyte ratio with age and 180-day mortality after emergency surgery
- PMID: 39289610
- PMCID: PMC11406743
- DOI: 10.1186/s12871-024-02718-z
Association of neutrophil-to-lymphocyte ratio with age and 180-day mortality after emergency surgery
Abstract
Background: To examine the relationship between neutrophil-to-lymphocyte ratio (NLR), age, and mortality rates after emergency surgery.
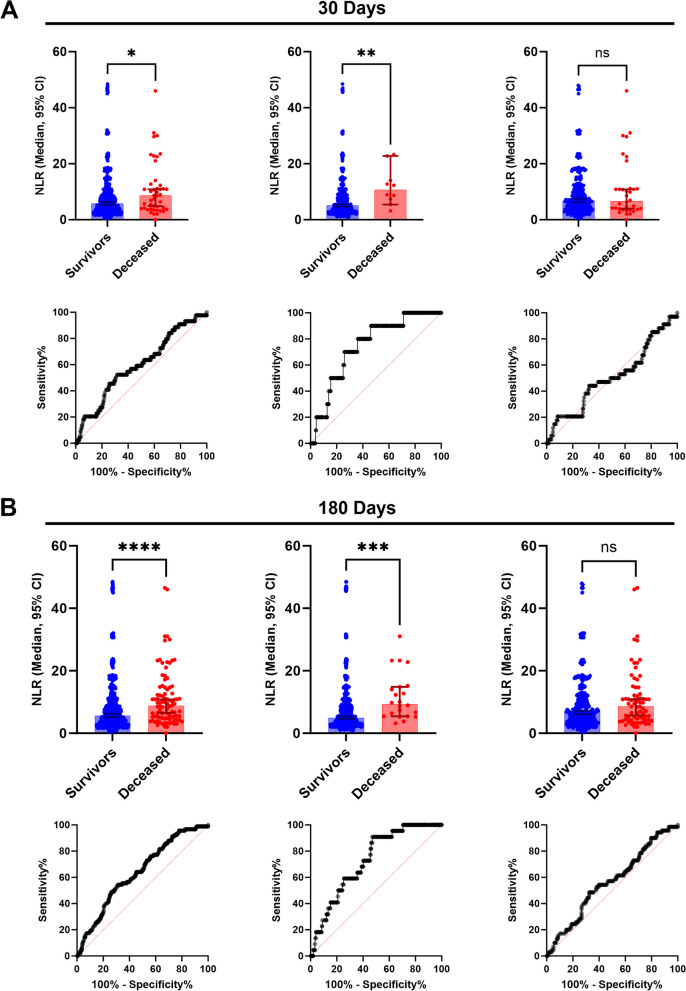
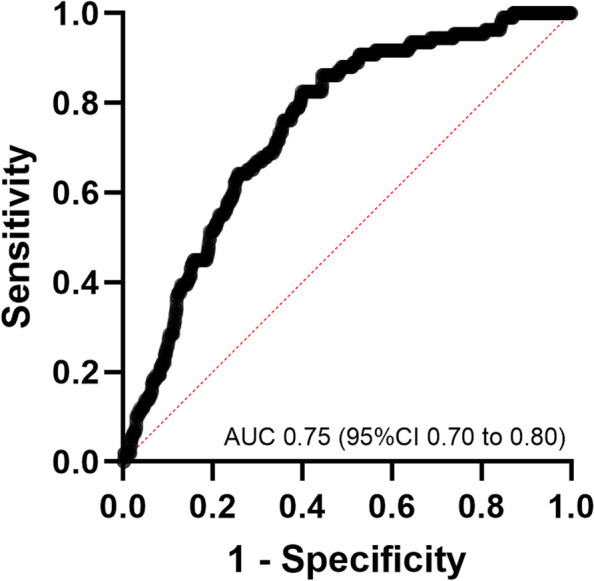
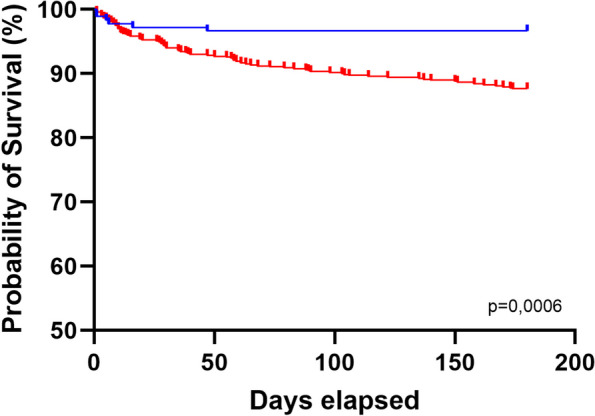
Methods: In this observational study, a total of 851 patients undergoing emergency surgery between January 2022 and January 2023 were retrospective examined. Using 30 and 180 days mortality data, NLR differences and receiver operating characteristic (ROC) curves were analyzed using a 65-year threshold. A multiple logistic regression model was constructed incorporating age and NLR. Finally, Kaplan-Meier curves were constructed for mortality.
Results: Among 851 patients, the 30 and 180 days mortality rates were 5.2% and 10.8%, respectively. Median NLR in 30 days was 5.6 (3.1 to 9.6) in survivors and 8.7 (4.6 to 13.4) in deceased patients (p < 0.0001); in 180 days, it was 5.5 (3.1 to 9.8) and 8.8 (4.8 to 14.5), respectively (p < 0.0001). In the 30- and 180-days mortality analyses, median NLRs were 5.1 (2.9 to 8.9) and 4.9 (2.9 to 8.8) in survivors and 10.6 (6.9 to 16.6) and 9.3 (5.4 to 14.9) in deceased patients aged < 65 years, respectively. The ROC AUC in patients younger than 65 years was higher for 30 days (AUC 0.75; 95% CI 0.72 to 0.87) and 180 days (AUC 0.73; 95% CI 0.64 to 0.81). Multivariate logistic regression revealed that the NLR (odds ratio, 1.03 [95% CI 1.005 to 1.053; p = 0.0133) and age (odds ratio, 1.05 [95% CI 1.034 to 1.064; p < 0.0001) significantly contributed to the model. Survival analysis revealed differences in the 180 days mortality (p = 0.0006).
Conclusion: We observed differences in preoperative NLR between patients who survived and those who died after emergency surgery. Age impacts the use of NLR as a mortality risk factor.
Trial registration: NCT06549101, retrospectively registered.
Keywords: Anesthesia; Emergency surgery; Mortality; Neutrophil-to-lymphocyte ratio; Prediction; Preoperative care.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
