

Iatrogenic pediatric unilateral vocal cord paralysis after cardiac surgery: a review
- PMID: 39290595
- PMCID: PMC11405229
- DOI: 10.3389/fped.2024.1460342
Iatrogenic pediatric unilateral vocal cord paralysis after cardiac surgery: a review
Abstract
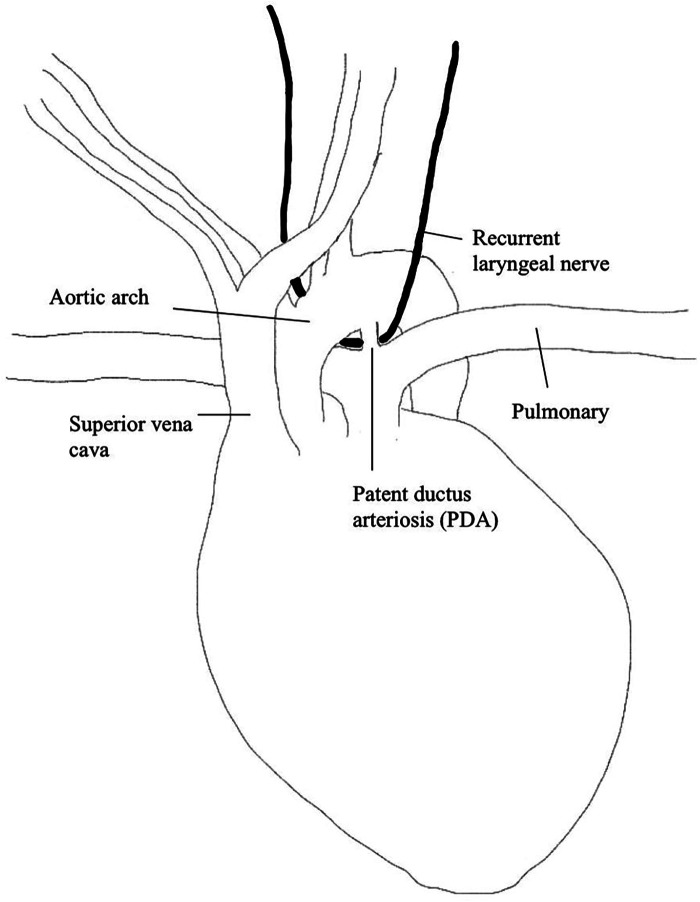
Unilateral vocal cord paralysis (UVCP) is a growing area of research in pediatrics as it spans across many specialties including otolaryngology, cardiology, general surgery, respirology, and speech language pathology. Iatrogenic injury is the most common cause of UVCP, however there is a wide range of data reporting the prevalence, symptom burden, and best treatment practice for this condition. The literature included systematic reviews and meta-analyses, retrospective studies and limited prospective studies. Overall, the literature lacked consistency in the diagnosis, treatment, and long-term outcomes of patients with UVCP. Many articles conflated bilateral vocal cord paralysis (BVCP) with UVCP and had limited data on the natural history of the condition. There was no consensus on objective and subjective measurements to evaluate the condition or best indications for requiring surgical intervention. Thyroplasty, injection medialization (IM) and recurrent laryngeal nerve reinnervation (RLNR) were the reported surgical interventions used to treat UVCP, however there was limited data on short and long-term surgical outcomes in children. More research is needed to determine the true prevalence, natural history, indications for surgical intervention and long-term outcomes for pediatric patients with this condition.
Keywords: cardiac surgery; laryngeal mobility disorders; laryngeal reinnervation; otolaryngology; pediatric surgery; pediatrics; unilateral vocal cord paralysis; vocal cord paralysis.
© 2024 Callaghan, El-Hakim and Isaac.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources