

The Sling Technique for Laparoscopic Liver Mobilization
- PMID: 39290722
- PMCID: PMC11406476
- DOI: 10.4293/JSLS.2024.00011
The Sling Technique for Laparoscopic Liver Mobilization
Abstract
Background: As liver surgery continues to evolve, be it open, laparoscopic or robotic, it remains a procedure that can deteriorate in the blink of an eye. Liver surgery in patients with hepatoma is further complicated, as the vast majority have significant fibrosis, if not cirrhosis. Thus, parenchymal sparing resection is increasingly necessary. Effective and safe intracorporeal mobilization of the liver is essential for minimal access parenchymal-sparing and conventional resection.
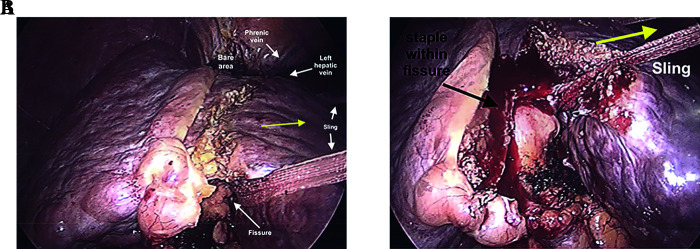
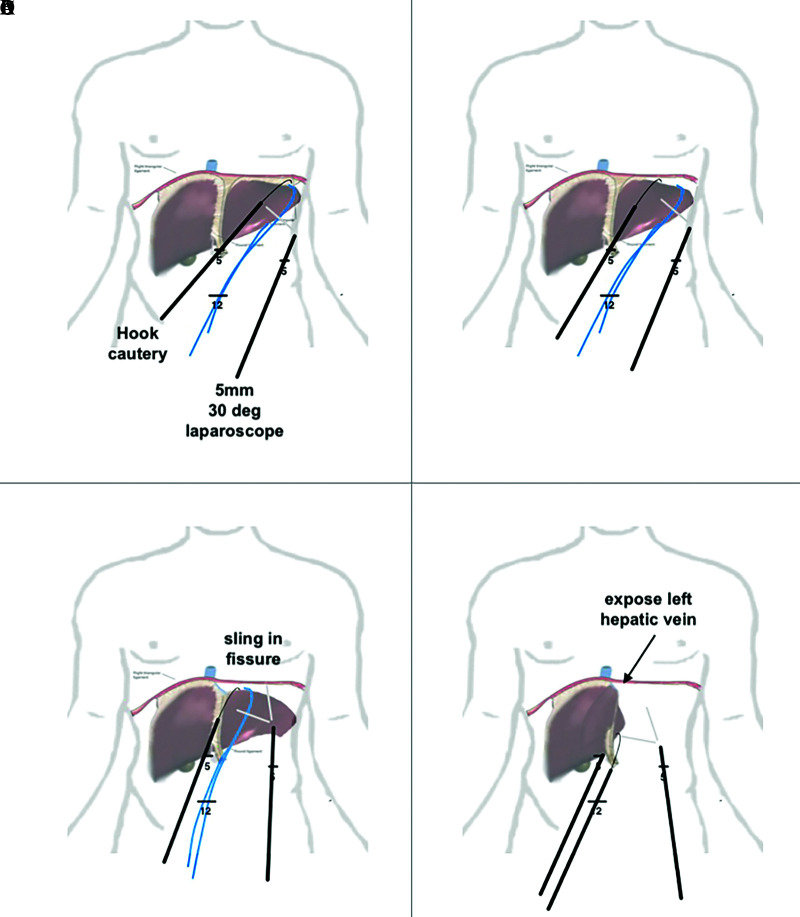
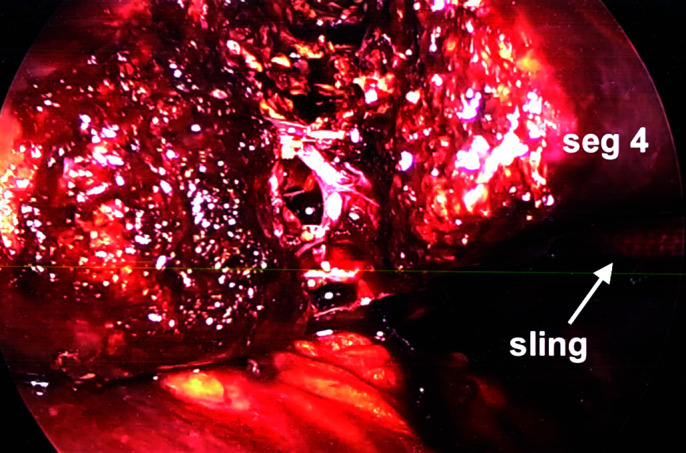
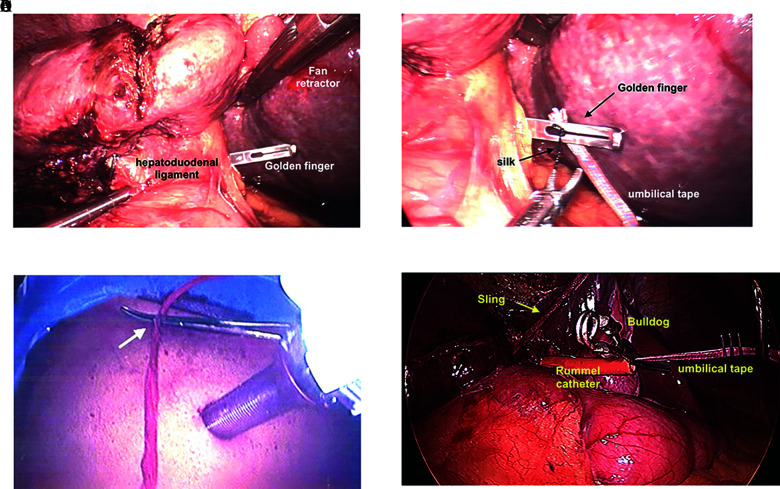
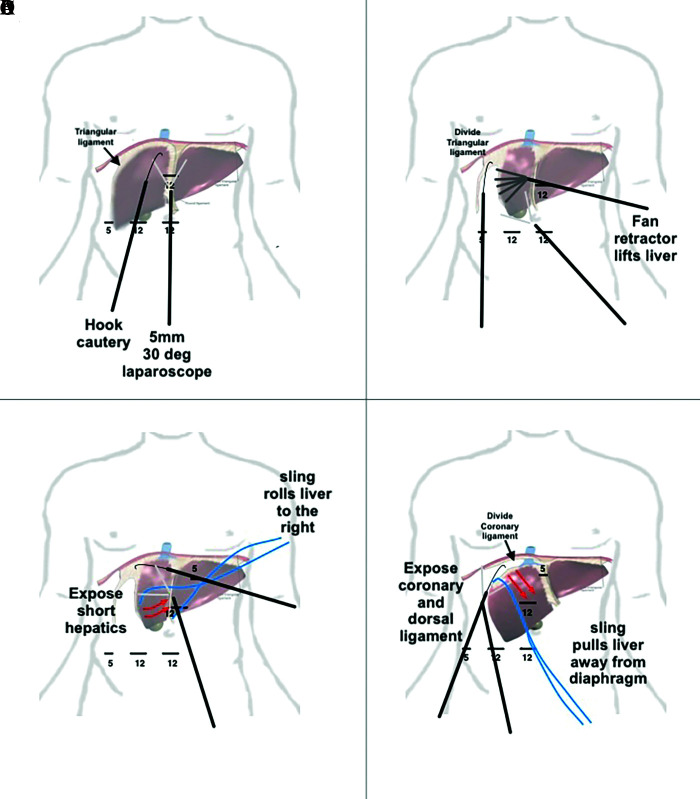
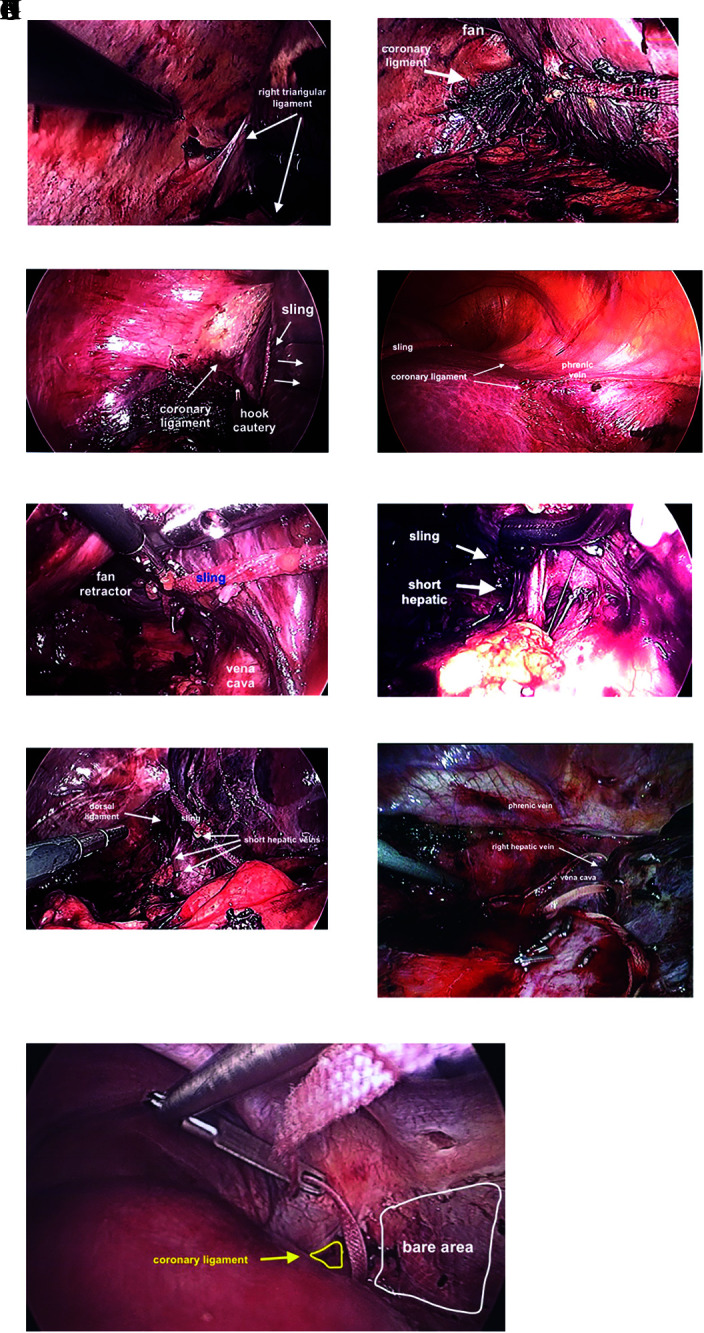
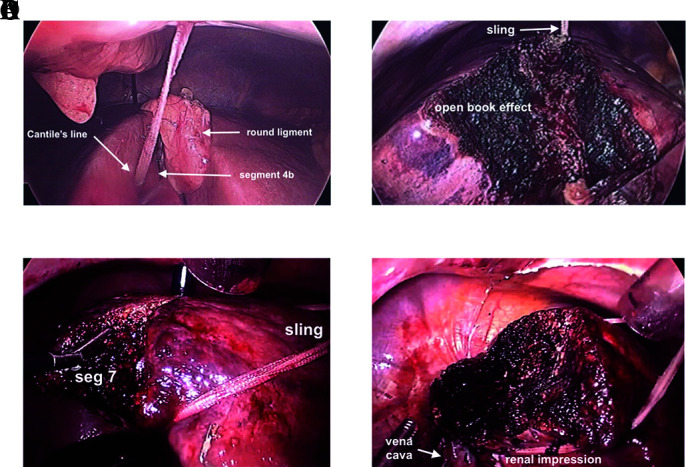
Methods: This retrospective review of over 150 cases performed provides a hands-on approach to laparoscopic hepatic mobilization with the use of an inexpensive technique using a 1" packing tape to "Sling" the liver in-order to divide the ligaments holding the liver in place and optimally position the liver for parenchymal transection.
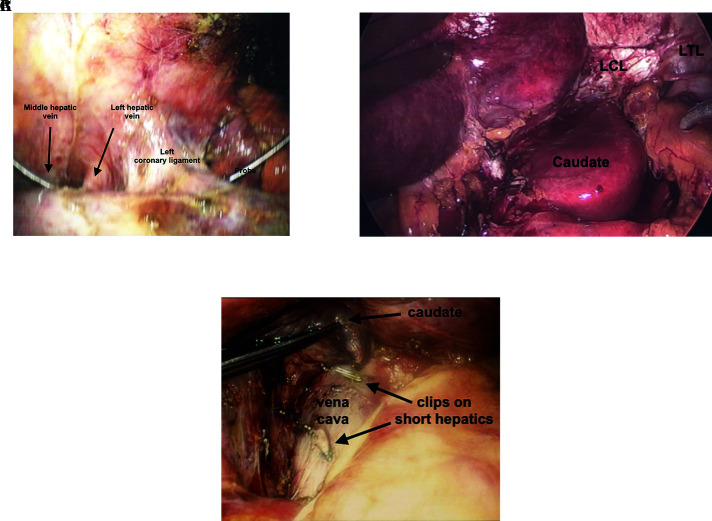
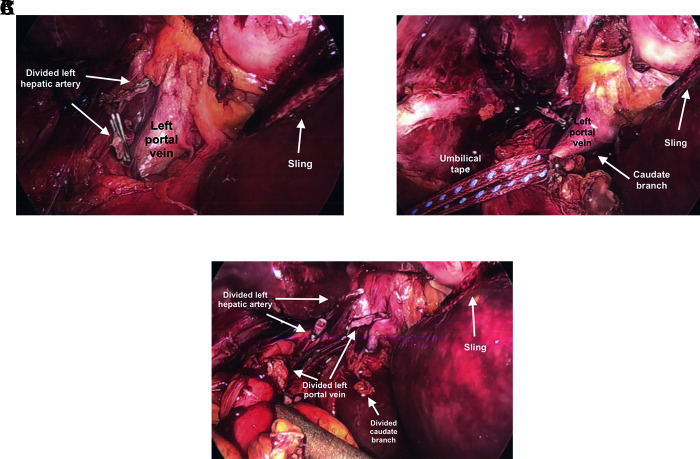
Results: Use of a 1" packing tape to "Sling" the liver intracorporeally is demonstrated to enable mobilization of the liver for tissue sparing non-anatomic, anatomic and major resections.
Conclusion: Use of a 1" packing tape to "Sling" the liver intracorporeally can facilitate mobilization for resection. Surgeons hoping to master minimal access resection should also be well versed in the use of laparoscopic ultrasound and liver transplant "Piggyback" technique.
Keywords: Intracorporial liver mobilization; Laparoscopic liver resection.
© 2024 by SLS, Society of Laparoscopic & Robotic Surgeons.
Figures
References
-
- Buell JF, Cherqui D, Geller DA, et al. ; World Consensus Conference on Laparoscopic Surgery. The international position on laparoscopic liver surgery: the Louisville Statement, 2008. Ann Surg. 2009;250(5):825–830. - PubMed
-
- Lamadé W, Glombitza G, Fischer L, et al. The impact of 3-dimensional reconstructions on operation planning in liver surgery. Arch Surg. 2000;135(11):1256–1261. - PubMed
-
- Björnsson B, Lundgren L. A personal computer freeware as a tool for surgeons to plan liver resections. Scand J Surg. 2016;105(3):153–157. - PubMed
-
- Ielpo B, Pittau G, Ciacio O, et al. Standardized laparoscopic right hepatic lobe mobilization. J Hepatobiliary Pancreat Sci. 2022;29(5):e30–e32. - PubMed
-
- Choi SH, Choi GH, Han DH, Kwon SW, Choi JS. Laparoscopic right hepatectomy: toward protocolization and simplification. Ann Surg Oncol. 2017;24(2):554–555. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials