

Impact of the Noninvasive Diagnostic Algorithm on Clinical Presentation and Prognosis in Cardiac Amyloidosis
- PMID: 39290816
- PMCID: PMC11405895
- DOI: 10.1016/j.jacadv.2024.101232
Impact of the Noninvasive Diagnostic Algorithm on Clinical Presentation and Prognosis in Cardiac Amyloidosis
Abstract
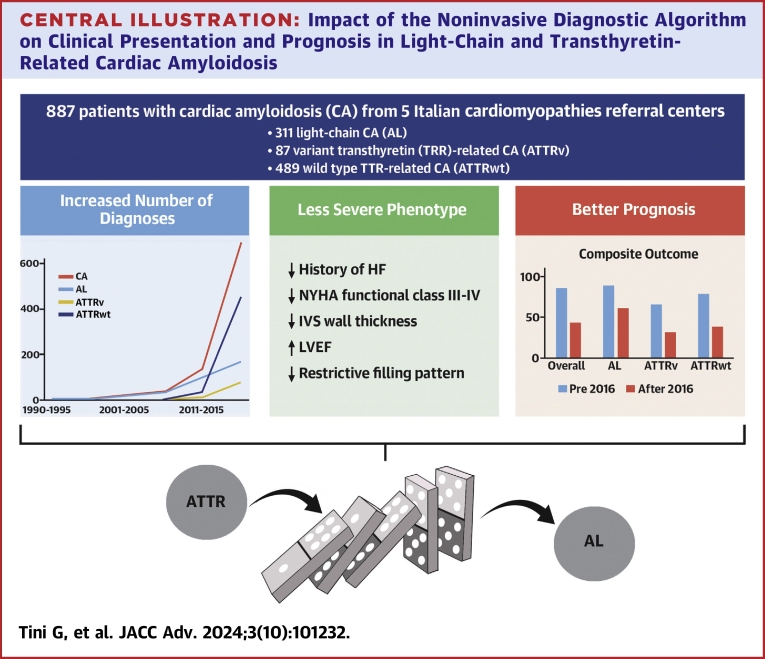
Background: The introduction of a noninvasive diagnostic algorithm in 2016 led to increased awareness and recognition of cardiac amyloidosis (CA).
Objectives: The purpose of this study was to analyze the impact of the introduction of the noninvasive diagnostic algorithm on diagnosis and prognosis in a multicenter Italian CA cohort.
Methods: This was a retrospective analysis of 887 CA patients from 5 Italian Cardiomyopathies Referral Centers: 311 light-chain CA, 87 variant transthyretin (TTR)-related CA, 489 wild-type TTR-related CA. Clinical characteristics and outcomes (all-cause mortality and heart failure [HF] hospitalizations) were compared overall and for each CA subtype between patients diagnosed before versus after 2016. Outcomes were further compared by propensity score weighted Kaplan-Meier analysis and Cox regression analysis.
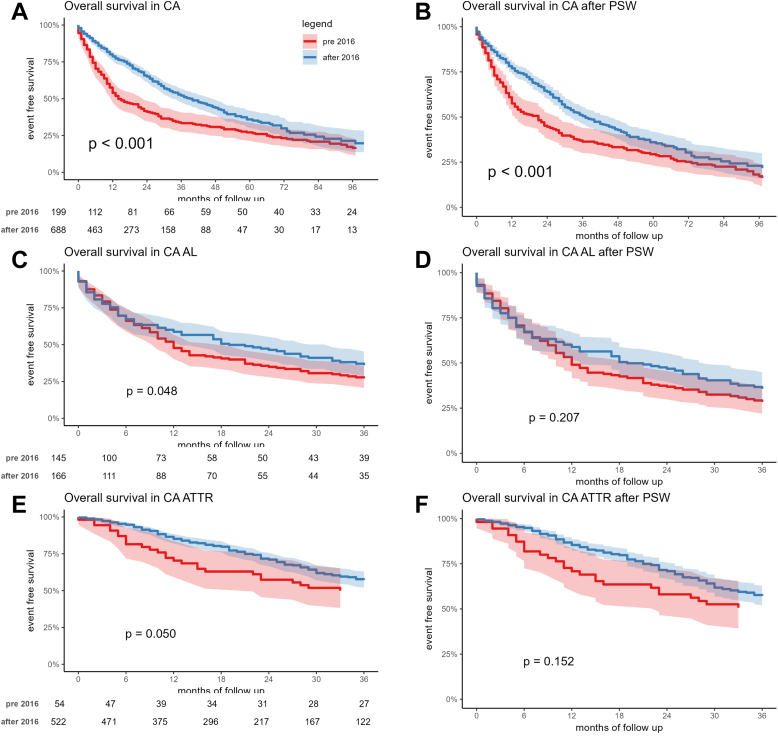
Results: CA diagnoses increased after 2016, in particular for wild-type TTR-related CA. Patients diagnosed after versus before 2016 were older, had less frequently a history of HF prior to diagnosis, and NYHA functional class III-IV at diagnosis. Over a median follow-up of 18 months, 172 (86%) patients diagnosed before 2016 died or had an HF hospitalization, versus 300 (44%) diagnosed after 2016. Propensity score weighted Kaplan-Meier analysis showed worse outcomes (P < 0.001) for patients diagnosed before 2016. At Cox regression analysis, CA diagnosis after 2016 was an independent protective factor for the composite outcome (HR: 0.69; P = 0.001), with interaction by CA subtype (significant in TTR-related CA and null in light-chain).
Conclusions: CA patients diagnosed after 2016 showed a less severe phenotype and a better prognosis. The impact of the noninvasive diagnostic algorithm on outcomes was particularly relevant in TTR-related CA.
Keywords: AL cardiac amyloidosis; cardiac amyloidosis; heart failure; noninvasive diagnosis; transthyretin cardiac amyloidosis.
© 2024 The Authors.
Conflict of interest statement
The work reported in this publication was funded by the 10.13039/501100003196Italian Ministry of Health, RC-2022-2773270 project. The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures


References
-
- Gillmore J.D., Maurer M.S., Falk R.H., et al. Nonbiopsy diagnosis of cardiac transthyretin amyloidosis. Circulation. 2016;133:2404–2412. - PubMed
-
- Barrett C.D., Dobos K., Liedtke M., et al. A changing landscape of mortality for systemic light chain amyloidosis. JACC Heart Fail. 2019;7:958–966. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
