

Importance of IFT140 in Patients with Polycystic Kidney Disease Without a Family History
- PMID: 39291187
- PMCID: PMC11403091
- DOI: 10.1016/j.ekir.2024.06.021
Importance of IFT140 in Patients with Polycystic Kidney Disease Without a Family History
Abstract
Introduction: Recently, the monoallelic loss-of-function IFT140 variant was identified as a causative gene for autosomal dominant polycystic kidney disease (ADPKD). In patients with polycystic kidneys who have a positive family history, >90% have pathogenic variants in PKD1 or PKD2, whereas only 1% have IFT140. However, approximately 40% of patients with polycystic kidneys without a family history do not have any pathogenic variants in PKD1 and PKD2.
Methods: We conducted a comprehensive genetic analysis of 157 adult patients with polycystic kidneys whose parents did not have evident polycystic kidneys. We sequenced up to 92 genes associated with inherited cystic kidney disease, including IFT140.
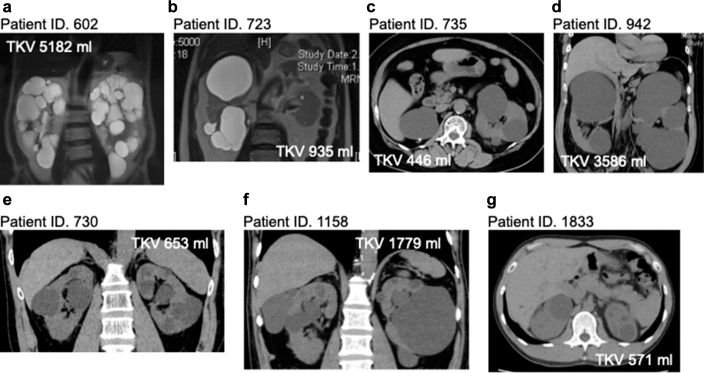
Results: Of the 157 patients, 7 (4.5%) presented with monoallelic loss-of-function variants in the IFT140 gene, 51 (32.5%) with pathogenic variants in the PKD1 or PKD2 gene, and 7 (4.5%) with pathogenic variants in other genes related to inherited kidney cystic disease. The proportion of monoallelic loss-of-function IFT140 variants in this cohort was higher than that in previously reported cohorts with polycystic kidneys who had a positive family history. None of the patients with monoallelic loss-of-function IFT140 variants had polycystic liver disease (PLD). Furthermore, patients with IFT140 pathogenic variants had a significantly smaller kidney volume and a remarkably higher estimated glomerular filtration rate (eGFR) than those with PKD1 pathogenic variants (P = 0.01 and 0.03, respectively).
Conclusion: Because the phenotype of polycystic kidneys caused by the IFT140 gene is mild, parental kidney disease may be overlooked. Therefore, patients without a positive family history are more likely to carry pathogenic variants in IFT140.
Keywords: ADPKD; IFT140; inherited kidney cystic disease; next-generation sequencing; polycystic kidney disease; total kidney volume.
© 2024 International Society of Nephrology. Published by Elsevier Inc.
Figures



References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
