

Kidney Biopsy Findings After Lung Transplantation
- PMID: 39291190
- PMCID: PMC11403037
- DOI: 10.1016/j.ekir.2024.07.005
Kidney Biopsy Findings After Lung Transplantation
Abstract
Introduction: The early diagnosis of histological kidney damage after lung transplantation (LT) is of paramount importance given the negative prognostic implications of kidney disease.
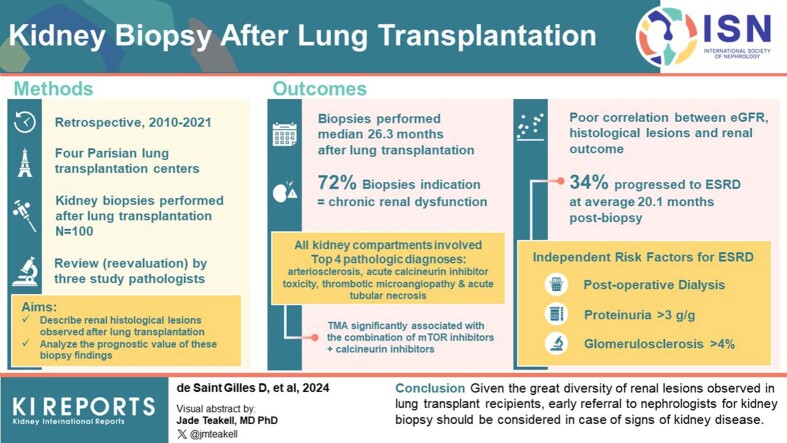
Methods: Three pathologists analyzed all kidney biopsies (KBs) (N = 100) performed from 2010 to 2021 on lung transplant patients in 4 Paris transplantation centers.
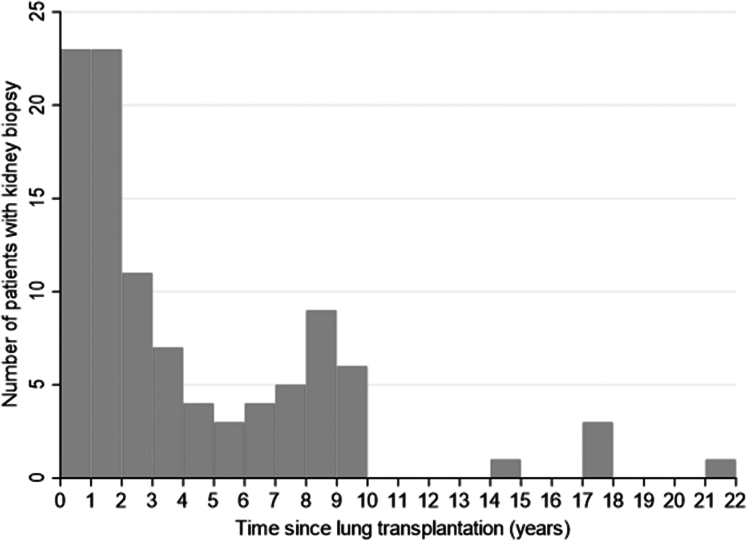
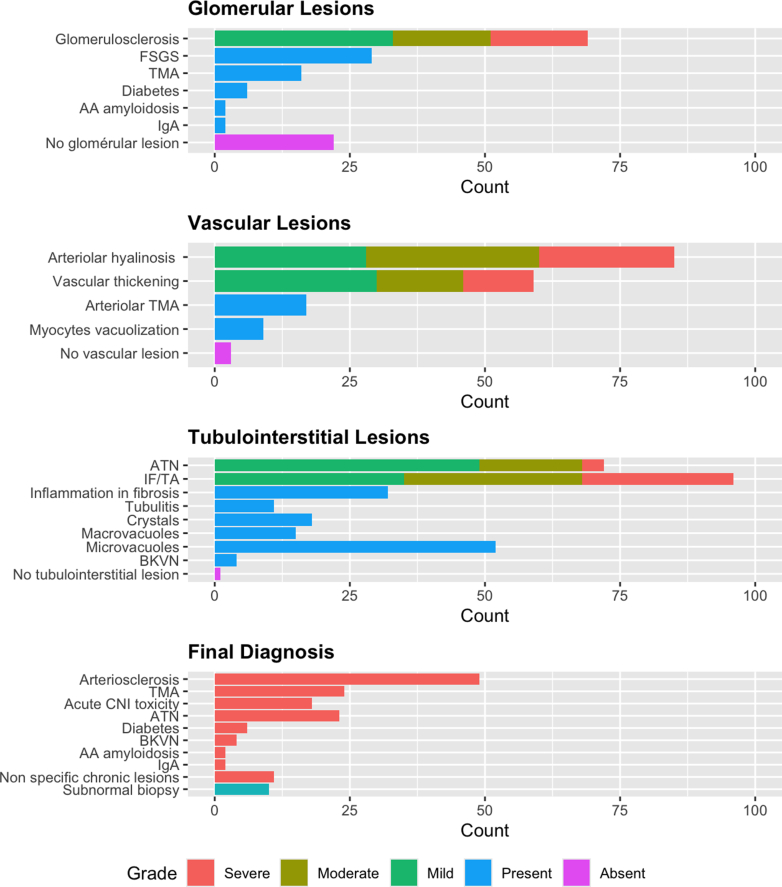
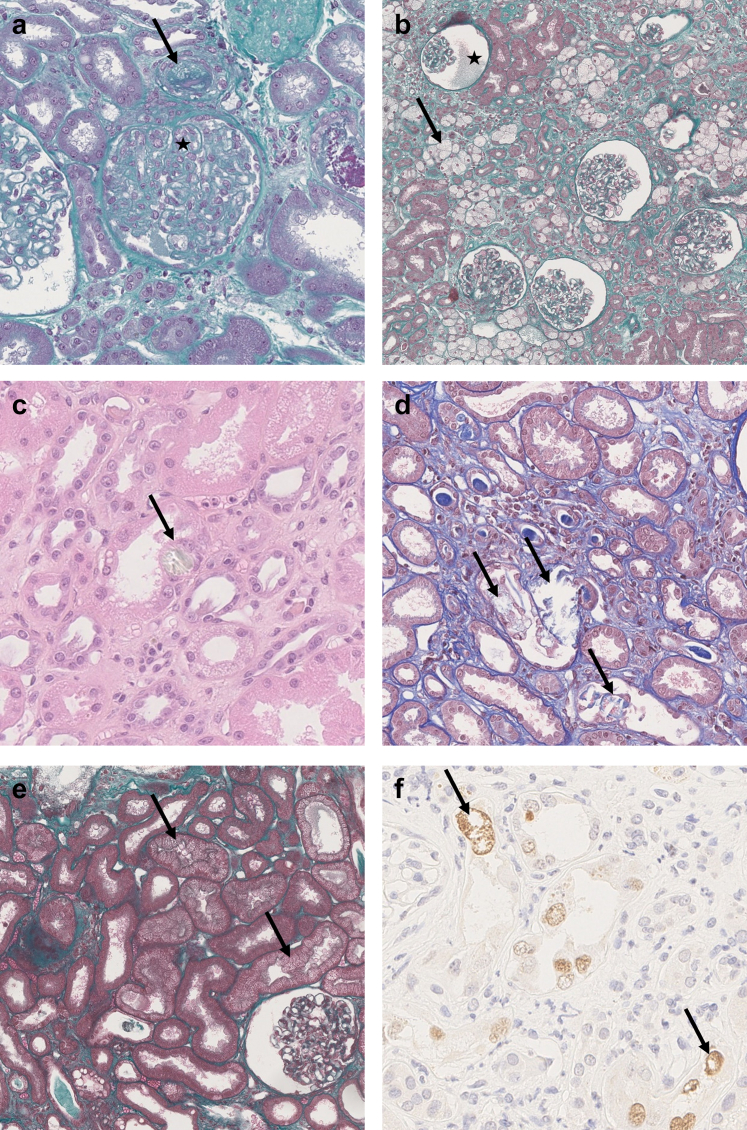
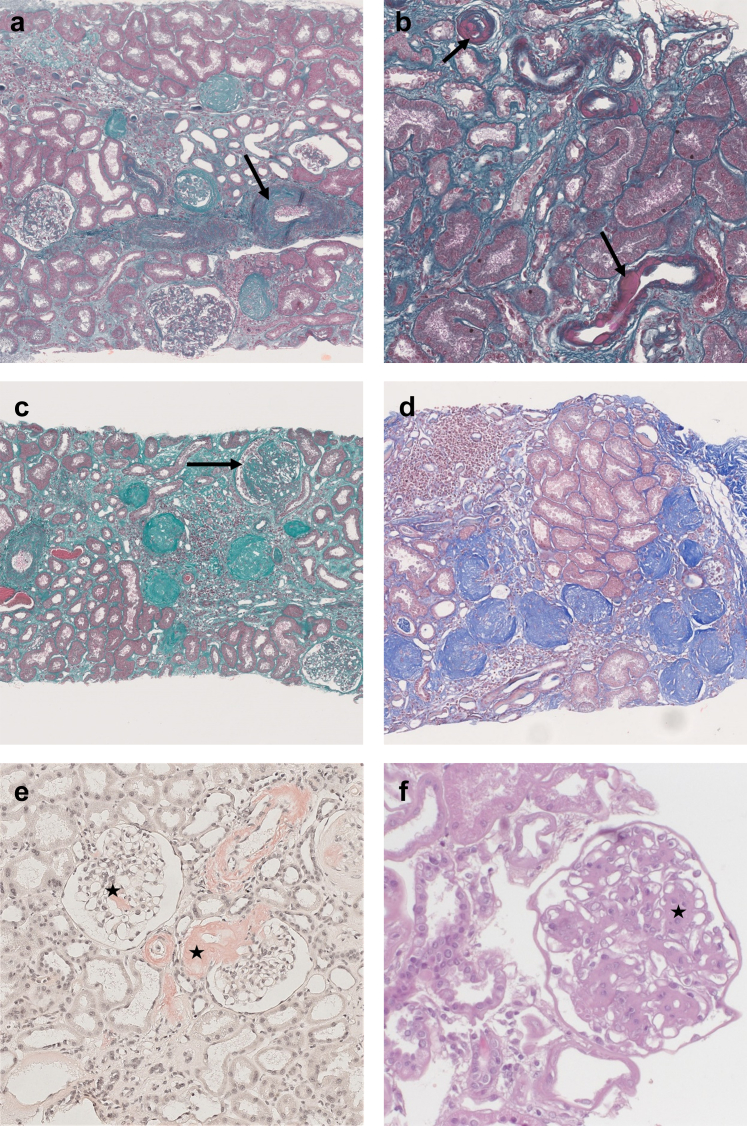
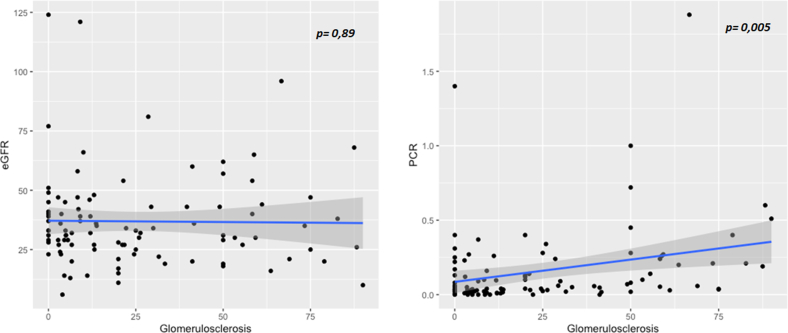
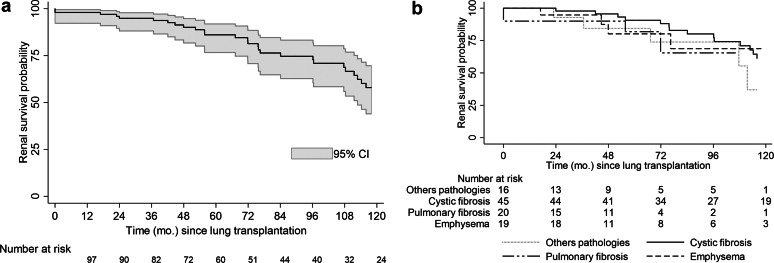
Results: The main indication for biopsy was chronic renal dysfunction (72% of patients). Biopsies were performed at a median of 26.3 months after transplantation and 15 months after a decline in estimated glomerular filtration rate (eGFR) or the onset of proteinuria. Biopsies revealed a wide spectrum of chronic lesions involving the glomerular, vascular, and tubulointerstitial compartments. The 4 most frequent final diagnoses, observed in 18% to 49% of biopsies, were arteriosclerosis, acute calcineurin inhibitor (CNI) toxicity, thrombotic microangiopathy (TMA) and acute tubular necrosis (ATN). TMA was significantly associated with a combination of mTOR inhibitors (mTORi) or CNIs with biological signs present in only 50% of patients. The eGFR was poorly correlated with most lesions, particularly percent glomerulosclerosis, and with the risk of end-stage renal disease (ESRD). Thirty-four patients progressed to ESRD at an average of 20.1 months after biopsy. Three factors were independently associated with the risk of ESRD: postoperative dialysis, proteinuria >3 g/g and percent glomerulosclerosis >4%.
Conclusion: Given the great diversity of renal lesions observed in lung transplant recipients, early referral to nephrologists for KB should be considered for these patients when they present with signs of kidney disease.
Keywords: acute kidney injury; calcineurin inhibitor toxicity; chronic kidney disease; kidney pathology; lung transplantation; thrombotic microangiopathy.
© 2024 International Society of Nephrology. Published by Elsevier Inc.
Figures
References
-
- Rapport Agence de la Biomédecine 2021. https://rams.agence-biomedecine.fr/greffe-cardio-pulmonaire-et-pulmonaire-0
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
