

Combination of Cardiovascular, Kidney, and Metabolic Diseases in a Syndrome Named Cardiovascular-Kidney-Metabolic, With New Risk Prediction Equations
- PMID: 39291205
- PMCID: PMC11403032
- DOI: 10.1016/j.ekir.2024.05.033
Combination of Cardiovascular, Kidney, and Metabolic Diseases in a Syndrome Named Cardiovascular-Kidney-Metabolic, With New Risk Prediction Equations
Erratum in
-
Corrigendum to "Combination of Cardiovascular, Kidney, and Metabolic Diseases in a Syndrome Named Cardiovascular-Kidney-Metabolic, With New Risk Prediction Equations" [Kidney International Reports Volume 9, Issue 9, September 2024, Pages 2608-2618].Kidney Int Rep. 2025 Jan 3;10(3):977. doi: 10.1016/j.ekir.2025.01.002. eCollection 2025 Mar. Kidney Int Rep. 2025. PMID: 40225388 Free PMC article.
Abstract
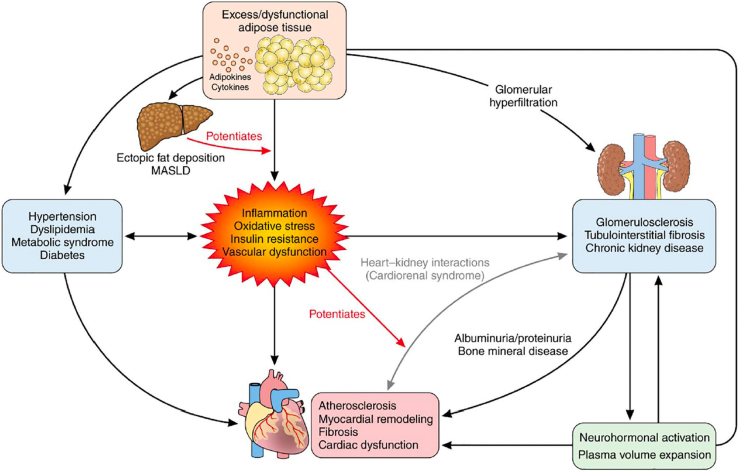
Associations of chronic kidney disease (CKD) with metabolic syndrome and cardiovascular disease (CVD) have long been recognized. Until recently, such associations were mainly limited to interrelationships between either heart and kidney, heart and metabolic syndrome, or metabolic syndrome and kidney. It is the merit of the American Heart Association (AHA) to have set up a work group of cardiologists, endocrinologists, and nephrologists for the purpose of combining all 3 disorders in a single entity, as an appreciation of their pathophysiological interrelatedness. To this end, they proposed the term cardiovascular-kidney-metabolic (CKM) syndrome, which reflects multidirectional relationships among metabolic risk factors, CKD, and the cardiovascular system. Following a consensus approach in defining CKM with 5 stages, the work group subsequently developed new risk prediction equations, named predicting risk of CVD events (PREVENT) equations, which included estimated glomerular filtration rate (eGFR) and albuminuria as variables in addition to traditional cardiovascular and metabolic factors. Despite several limitations, this development is a major step forward in cardiovascular risk prediction. Its clinical application should translate into earlier, more appropriate treatment and prevention of CKM syndrome.
Keywords: CKM syndrome; cardiovascular disease; kidney disease; metabolic syndrome; risk prediction.
© 2024 International Society of Nephrology. Published by Elsevier Inc.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
