

Serum Potassium in Thyroid Cancer Patients With Hypothyroidism During Thyroid Hormone Withdrawal: A Retrospective Study
- PMID: 39291259
- PMCID: PMC11406601
- DOI: 10.1177/11795514241278519
Serum Potassium in Thyroid Cancer Patients With Hypothyroidism During Thyroid Hormone Withdrawal: A Retrospective Study
Abstract
Background: Several case reports and a few studies have reported that hypothyroid patients have elevated serum potassium levels. However, hypothyroidism has not been widely accepted as a cause of hyperkalemia.
Objectives: This study aims to evaluate the incidence of hyperkalemia and factors influencing serum potassium levels in thyroid cancer patients with hypothyroidism during thyroid hormone withdrawal before radioactive iodine (RAI) treatment.
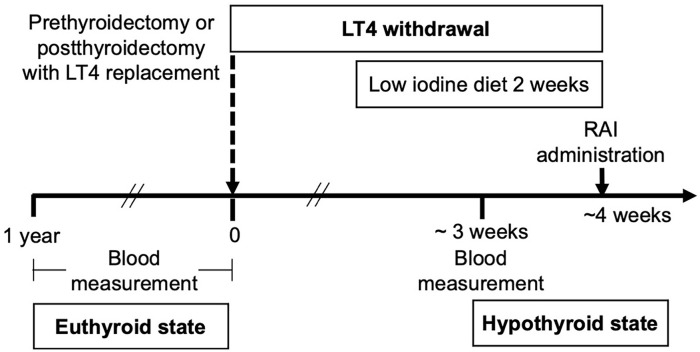
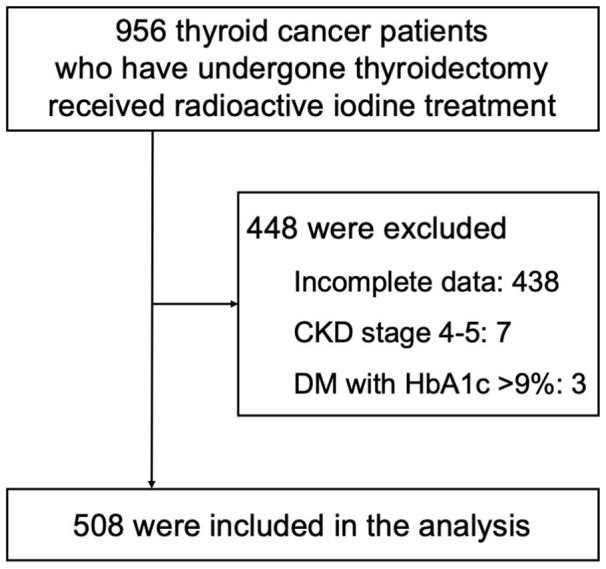
Methods: We conducted a retrospective review of electronic medical records from January 2017 to June 2021, involving 956 thyroid cancer patients post-thyroidectomy and undergoing RAI. Laboratory parameters, including serum potassium levels, were collected in both euthyroid (<1 year prior to RAI) and hypothyroid states.
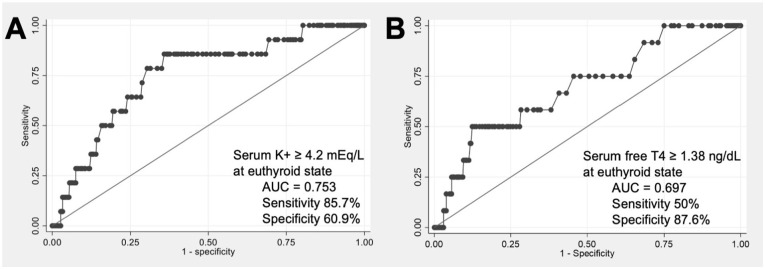
Results: Among 508 patients (mean age 52 years, 79.3% female), hyperkalemia (potassium ⩾ 5.0 mEq/L) occurred in 2.8%, without severe hyperkalemia (potassium ⩾ 6.5 mEq/L). The hypothyroid state exhibited significantly higher serum potassium than the euthyroid state [4.16 (IQR, 3.94-4.41) vs 4.10 (IQR, 3.90-4.35) mEq/L, P < .01]. The mean change in potassium levels between the euthyroid and hypothyroid state was 0.05 ± 0.17 mEq/L. Pre-thyroid hormone withdrawal (euthyroid state) factors associated with serum potassium levels in the hypothyroid state included age, use of angiotensin-converting enzyme inhibitors, diabetes mellitus, serum BUN/creatinine, serum potassium levels, hemoglobin A1c (positive correlation); and thiazide use and eGFR (negative correlation). In the hypothyroid state, hyperkalemia was more likely in patients with serum potassium ⩾4.2 mEq/L (OR 9.36, P < .01) or free T4 ⩾1.38 ng/dL (OR 7.05, P < .01) during the euthyroid state.
Conclusions: The incidence of hyperkalemia was low in our hypothyroid cohorts. However, physicians should remain vigilant for cases with risk factors for developing hyperkalemia.
Keywords: Electrolyte; hyperkalemia; hypothyroidism; iodine radioisotopes; thyroid neoplasms; water-electrolyte imbalance.
Plain language summary
Serum Potassium in Hypothyroid Patients A retrospective cohort study of thyroid cancer patients undergoing radioactive iodine therapy found a low incidence of hyperkalemia (2.8%) during hypothyroidism. Patients exhibited higher serum potassium levels, influenced by factors included age, medication use (ACEI), diabetes mellitus, and initial potassium levels. Elevated initial potassium and thyroid hormone levels were associated with higher risk of hypothyroid-related hyperkalemia. Physicians should remain vigilant for hyperkalemia in these patients, particularly those with predisposing factors, warranting further mechanistic studies and broader validations.
© The Author(s) 2024.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Hyperkalemia develops in some thyroidectomized patients undergoing thyroid hormone withdrawal in preparation for radioactive iodine ablation for thyroid carcinoma.Endocr Pract. 2015 May;21(5):488-94. doi: 10.4158/EP14532.OR. Epub 2015 Feb 9. Endocr Pract. 2015. PMID: 25667379
-
RENAL FUNCTION AND PLASMA RENIN ACTIVITY AS POTENTIAL FACTORS CAUSING HYPERKALEMIA IN PATIENTS WITH THYROID CARCINOMA UNDERGOING THYROID HORMONE WITHDRAWAL FOR RADIOACTIVE IODINE THERAPY.Endocr Pract. 2020 Feb;26(2):197-206. doi: 10.4158/EP-2019-0374. Epub 2019 Oct 25. Endocr Pract. 2020. PMID: 31652100
-
Prevalence and severity of hyponatremia and hypercreatininemia in short-term uncomplicated hypothyroidism.J Endocrinol Invest. 1999 Jan;22(1):35-9. doi: 10.1007/BF03345476. J Endocrinol Invest. 1999. PMID: 10090135
-
Risk factors for developing hyponatremia in thyroid cancer patients undergoing radioactive iodine therapy.PLoS One. 2014 Aug 29;9(8):e106840. doi: 10.1371/journal.pone.0106840. eCollection 2014. PLoS One. 2014. PMID: 25170831 Free PMC article.
-
Severe hyponatremia following radioactive iodine therapy in patients with differentiated thyroid cancer.Thyroid. 2014 Apr;24(4):773-7. doi: 10.1089/thy.2013.0110. Epub 2013 Nov 14. Thyroid. 2014. PMID: 24093878
References
-
- Liamis G, Filippatos TD, Liontos A, Elisaf MS. Management of endocrine disease: hypothyroidism-associated hyponatremia: mechanisms, implications and treatment. Eur J Endocrinol. 2017;176:R15-R20. - PubMed
-
- Benker G, Breuer N, Windeck R, Reinwein D. Calcium metabolism in thyroid disease. J Endocrinol Invest. 1988;11:61-69. - PubMed
-
- Wuttke H, Kessler FJ. [Clinical significance of serum magnesium concentration in thyrotoxicosis (author's transl)]. Med Klin. 1976;71:235-238. - PubMed
-
- Salih M, van Kinschot CMJ, Peeters RP, et al.. Thyrotoxic periodic paralysis: an unusual presentation of hyperthyroidism. Neth J Med. 2017;75:315-320. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
