

Levetiracetam versus carbamazepine monotherapy in the management of pediatric focal epilepsy: A systematic review and meta-analysis of randomized controlled trials
- PMID: 39292275
- PMCID: PMC11473619
- DOI: 10.1007/s00431-024-05768-0
Levetiracetam versus carbamazepine monotherapy in the management of pediatric focal epilepsy: A systematic review and meta-analysis of randomized controlled trials
Abstract
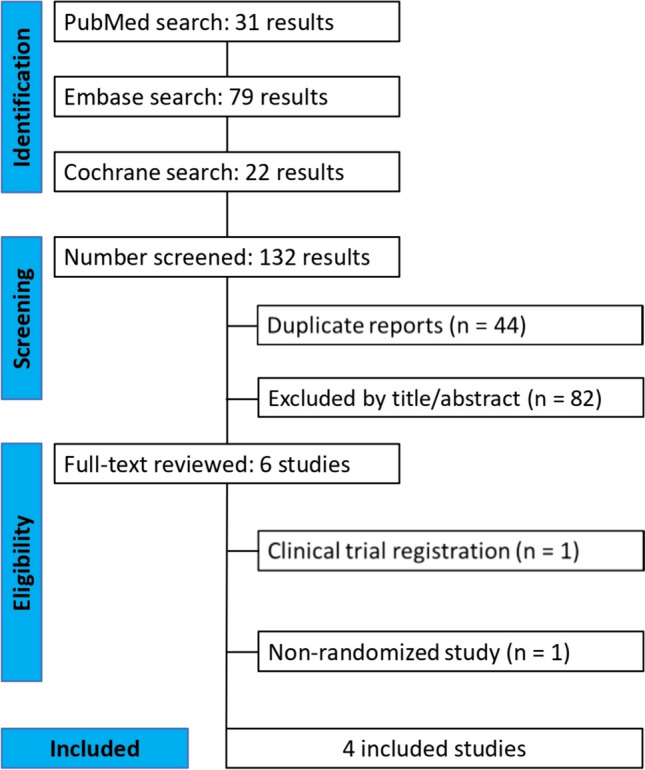
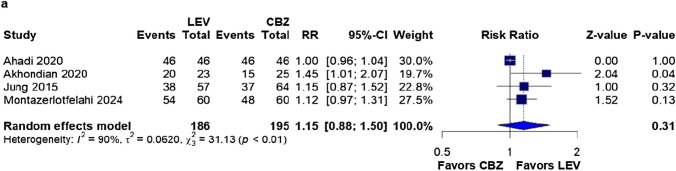
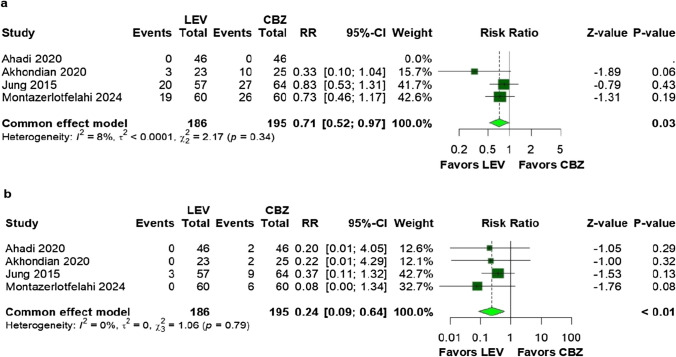
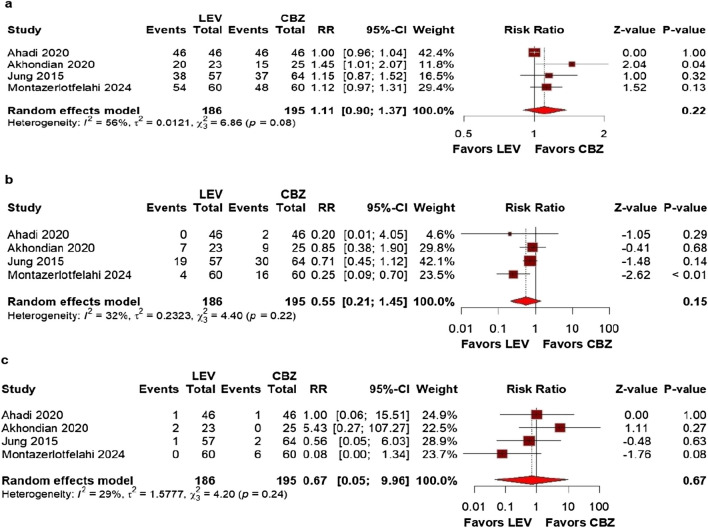
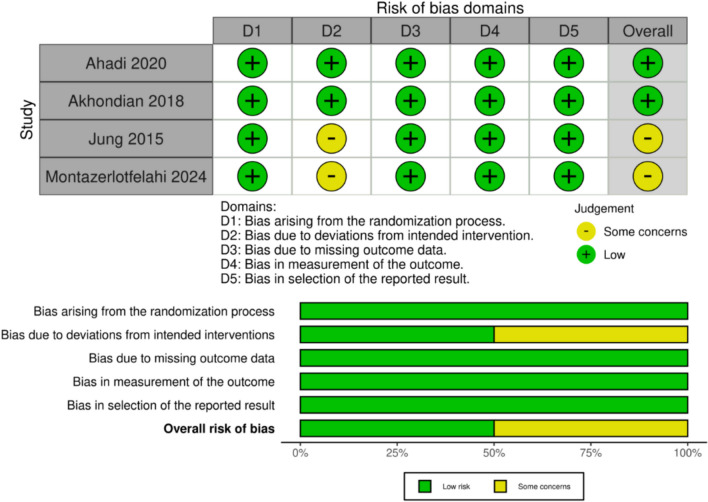
Levetiracetam (LEV) and carbamazepine (CBZ) are effective monotherapies for focal epilepsy in children. However, the best drug remains controversial. Therefore, we performed a systematic review and meta-analysis comparing LEV and CBZ monotherapy in the management of pediatric focal epilepsy (PFE). We searched PubMed, Embase, and Cochrane databases for randomized controlled trials (RCTs) published until February 2024 comparing LEV and CBZ monotherapy in PFE. Statistical analysis was performed using R version 4.2.2, heterogeneity was assessed using I2 statistics, and the risk of bias was evaluated using the RoB-2 tool. Risk Ratios (RR) with p < 0.05 were considered significant. The outcomes of interest were seizure freedom, any adverse events, adverse events leading to treatment discontinuation, dermatologic adverse events, and the frequency of at least one seizure, defined as the proportion of patients experiencing one or more seizures during the treatment period. Four RCTs comprising 381 children with a mean age of 7.32 to 9.28 years were included, of whom 186 (48.8%) received LEV monotherapy. There was no significant difference between groups (RR: 1.15; 95% CI 0.88-1.50; p = 0.31; I2 = 90%) regarding seizure freedom. The frequency of at least one seizure (RR: 0.71; 95% CI 0.52-0.97; p = 0.03; I2 = 8%) and dermatologic adverse events (RR: 0.24; 95% CI 0.09-0.64; p < 0.01; I2 = 0%) were both significantly lower in the LEV group. There were no significant differences in the presence of any adverse events (RR: 0.58; 95% CI 0.33-1.01; p = 0.05; I2 = 36%) or adverse events leading to treatment discontinuation (RR: 0.67; 95% CI 0.13-3.42; p = 0.63; I2 = 30%).Conclusion: In monotherapy, LEV was more advantageous than CBZ for PFE, with a lower frequency of seizures and fewer dermatological adverse events. However, both drugs are equally effective in achieving seizure freedom, adverse events without specification, and those that lead to treatment discontinuation. Our findings have important implications for clinical practice and decision-making in this condition.
Keywords: Carbamazepine; Focal epilepsy; Levetiracetam; Monotherapy; Pediatric.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests. All authors take responsibility for all aspects of the reliability and freedom from bias of the presented data and their interpretations.
Figures


References
-
- Banu SH, Jahan M, Koli UK, Ferdousi S, Khan NZ, Neville B (2007) Side effects of phenobarbital and carbamazepine in childhood epilepsy: randomised controlled trial. Bmj 334(7605):1207. 10.1136/bmj.39022.436389.BE - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
