

Year-Long Cannabis Use for Medical Symptoms and Brain Activation During Cognitive Processes
- PMID: 39292455
- PMCID: PMC11411392
- DOI: 10.1001/jamanetworkopen.2024.34354
Year-Long Cannabis Use for Medical Symptoms and Brain Activation During Cognitive Processes
Abstract
Importance: Cannabis is increasingly being used to treat medical symptoms, but the effects on brain function in those using cannabis for these symptoms are not known.
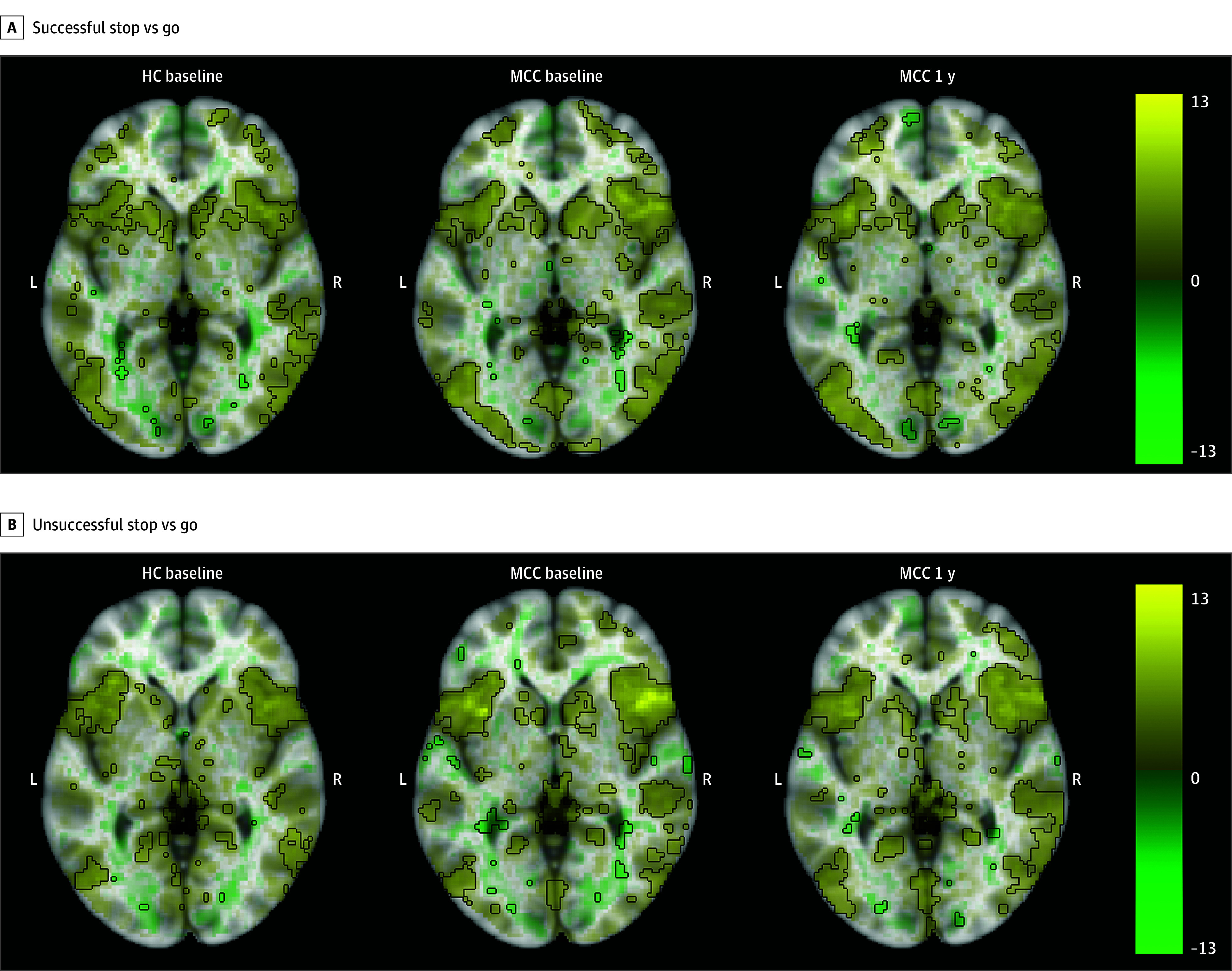
Objective: To test whether 1 year of cannabis use for medical symptoms after obtaining a medical cannabis card was associated with increased brain activation during working memory, reward, and inhibitory control tasks, areas of cognition affected by cannabis.
Design, setting, and participants: This cohort study was conducted from July 2017 to July 2020 among participants from the greater Boston area who were recruited as part of a clinical trial of individuals seeking medical cannabis cards for anxiety, depression, pain, or insomnia symptoms. Participants were aged between 18 and 65 years. Exclusion criteria were daily cannabis use and cannabis use disorder at baseline. Data analysis was conducted from August 2021 to April 2024.
Main outcomes and measures: Outcomes were whole brain functional activation during tasks involving working memory, reward, and inhibitory control at baseline and after 1 year of medical cannabis card ownership.
Results: Imaging was collected from participants before and 1 year after obtaining medical cannabis cards, with 57 participants at baseline (38 female [66.7%]; 6 [10.5%] Black and 45 [78.9%] White participants; 1 [1.8%] Hispanic participant; median [IQR] age, 34.0 [24.0-51.0] years) and 54 participants at 1 year (37 female [68.5%]; 4 [7.4%] Black and 48 [88.9%] White participants; 1 [1.9%] Hispanic participant, median [IQR] age, 36.5 [25.0-51.0] years). Imaging was also collected in 32 healthy control participants at baseline (22 female [68.8%]; 2 [6.2%] Black and 27 [84.4%] White participants; 3 [9.4%] Hispanic participants; median [IQR] age, 33.0 [24.8-38.2] years). In all groups and at both time points, functional imaging revealed canonical activations of the probed cognitive processes. No statistically significant difference in brain activation between the 2 time points (baseline and 1 year) in those with medical cannabis cards and no associations between changes in cannabis use frequency and brain activation after 1 year were found.
Conclusions and relevance: In this cohort study of adults obtaining medical cannabis cards for medical symptoms, no significant association between brain activation in the areas of cognition of working memory, reward, and inhibitory control and 1 year of cannabis use was observed. The results warrant further studies that probe the association of cannabis at higher doses, with greater frequency, in younger age groups, and with larger, more diverse cohorts.
Conflict of interest statement
Figures


Update of
-
Impact of year-long cannabis use for medical symptoms on brain activation during cognitive processes.medRxiv [Preprint]. 2024 May 1:2024.04.29.24306516. doi: 10.1101/2024.04.29.24306516. medRxiv. 2024. Update in: JAMA Netw Open. 2024 Sep 3;7(9):e2434354. doi: 10.1001/jamanetworkopen.2024.34354. PMID: 38746368 Free PMC article. Updated. Preprint.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
