

A systematic evaluation of the performance and properties of the UK Biobank Polygenic Risk Score (PRS) Release
- PMID: 39292644
- PMCID: PMC11410272
- DOI: 10.1371/journal.pone.0307270
A systematic evaluation of the performance and properties of the UK Biobank Polygenic Risk Score (PRS) Release
Abstract
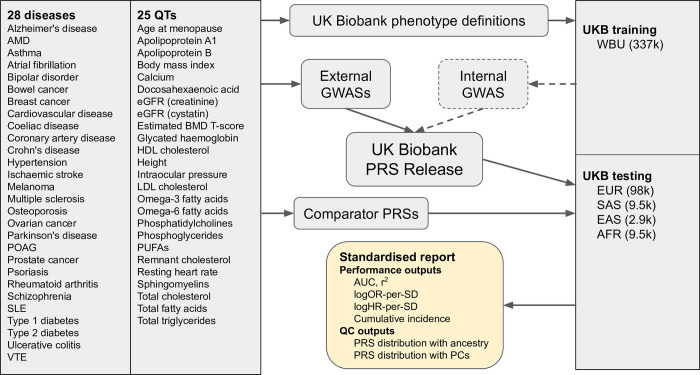
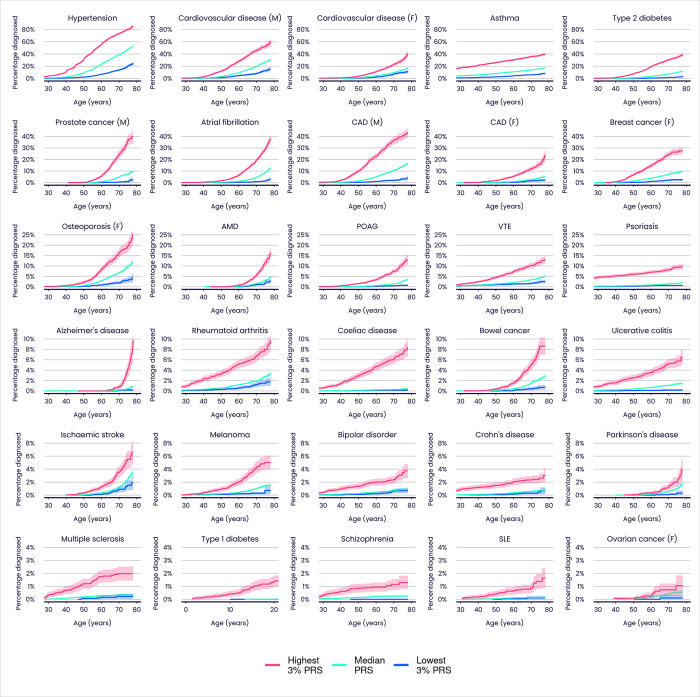
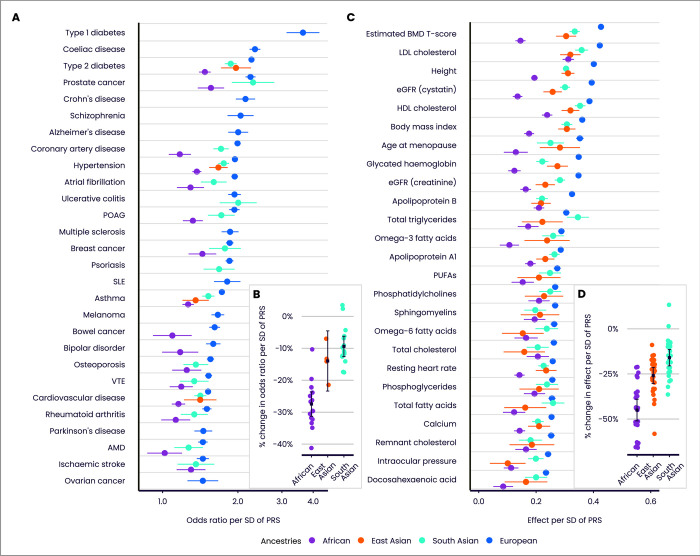
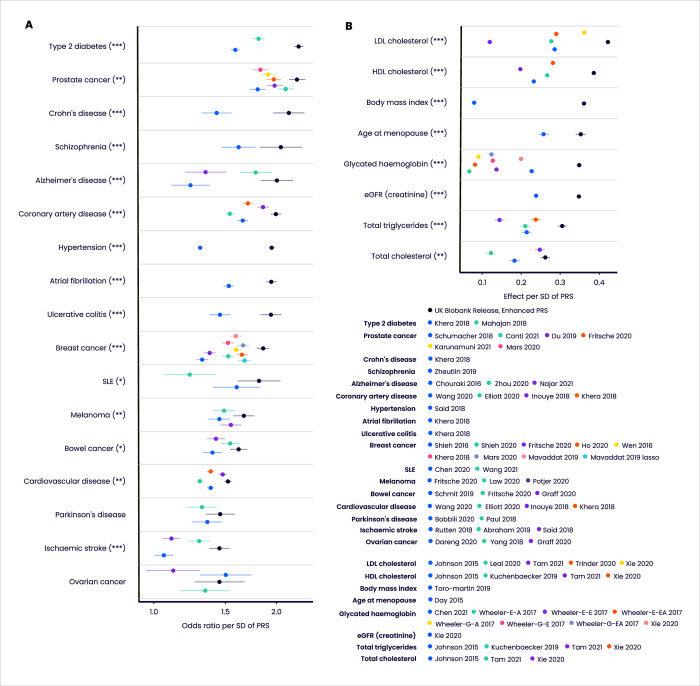
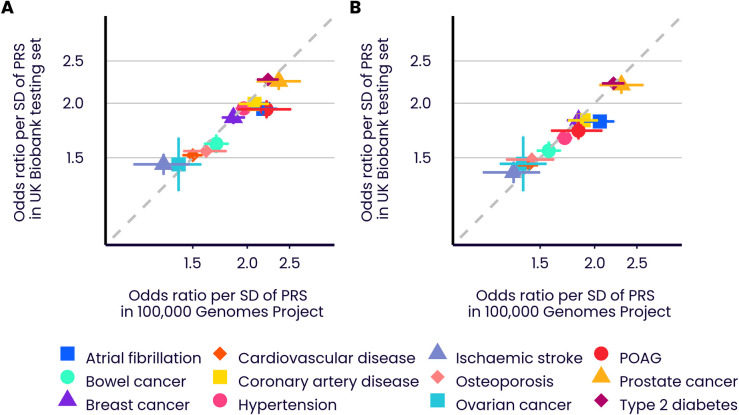
We assess the UK Biobank (UKB) Polygenic Risk Score (PRS) Release, a set of PRSs for 28 diseases and 25 quantitative traits that has been made available on the individuals in UKB, using a unified pipeline for PRS evaluation. We also release a benchmarking software tool to enable like-for-like performance evaluation for different PRSs for the same disease or trait. Extensive benchmarking shows the PRSs in the UKB Release to outperform a broad set of 76 published PRSs. For many of the diseases and traits we also validate the PRS algorithms in a separate cohort (100,000 Genomes Project). The availability of PRSs for 53 traits on the same set of individuals also allows a systematic assessment of their properties, and the increased power of these PRSs increases the evidence for their potential clinical benefit.
Copyright: © 2024 Thompson et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
Peter Donnelly and Gil McVean are partners in Peptide Groove LLP. Deborah Thompson, Daniel Wells, Saskia Selzam, Iliana Peneva, Rachel Moore, Kevin Sharp, William Tarran, Edward Beard,Fernando Riveros-Mckay, Carla Giner-Delgado, Duncan Palmer, Priyanka Seth, James Harrison, Gil McVean, Vincent Plagnol, Peter Donnelly and Michael Weale are current or former employees of Genomics plc, and are or have been in possession of stock or stock options for Genomics plc. Peter Donnelly and Gil McVean are Founders and Directors of Genomics plc, and Peter Donnelly is the CEO of Genomics plc. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
