

Phosphoproteomics predict response to midostaurin plus chemotherapy in independent cohorts of FLT3-mutated acute myeloid leukaemia
- PMID: 39293215
- PMCID: PMC11424955
- DOI: 10.1016/j.ebiom.2024.105316
Phosphoproteomics predict response to midostaurin plus chemotherapy in independent cohorts of FLT3-mutated acute myeloid leukaemia
Abstract
Background: Acute myeloid leukaemia (AML) is a bone marrow malignancy with poor prognosis. One of several treatments for AML is midostaurin combined with intensive chemotherapy (MIC), currently approved for FLT3 mutation-positive (FLT3-MP) AML. However, many patients carrying FLT3 mutations are refractory or experience an early relapse following MIC treatment, and might benefit more from receiving a different treatment. Development of a stratification method that outperforms FLT3 mutational status in predicting MIC response would thus benefit a large number of patients.
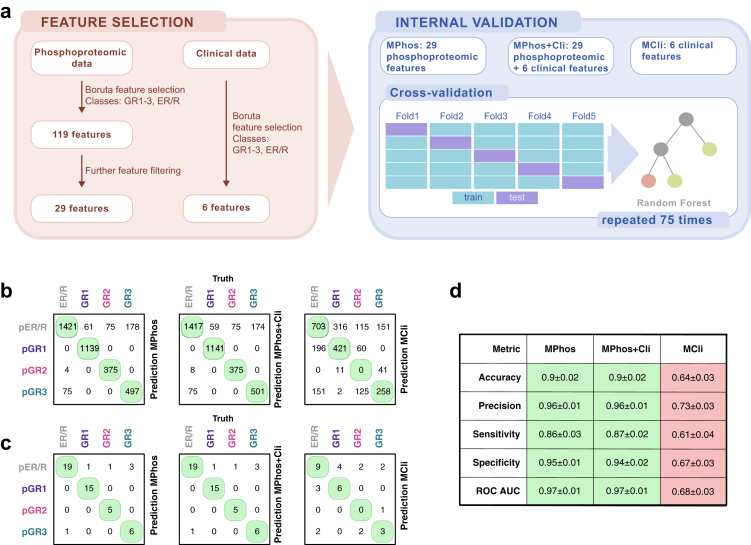
Methods: We employed mass spectrometry phosphoproteomics to analyse 71 diagnosis samples of 47 patients with FLT3-MP AML who subsequently received MIC. We then used machine learning to identify biomarkers of response to MIC, and validated the resulting predictive model in two independent validation cohorts (n = 20).
Findings: We identified three distinct phosphoproteomic AML subtypes amongst long-term survivors. The subtypes showed similar duration of MIC response, but different modulation of AML-implicated pathways, and exhibited distinct, highly-predictive biomarkers of MIC response. Using these biomarkers, we built a phosphoproteomics-based predictive model of MIC response, which we called MPhos. When applied to two retrospective real-world patient test cohorts (n = 20), MPhos predicted MIC response with 83% sensitivity and 100% specificity (log-rank p < 7∗10-5, HR = 0.005 [95% CI: 0-0.31]).
Interpretation: In validation, MPhos outperformed the currently-used FLT3-based stratification method. Our findings have the potential to transform clinical decision-making, and highlight the important role that phosphoproteomics is destined to play in precision oncology.
Funding: This work was funded by Innovate UK grants (application numbers: 22217 and 10054602) and by Kinomica Ltd.
Keywords: Acute myeloid leukaemia; Drug response prediction; Machine learning; Midostaurin plus chemotherapy; Phosphoproteomics; Precision medicine.
Copyright © 2024 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests WEB—is an employee at Kinomica, owns Kinomica share options, Kinomica funded attendance and travel to conferences, named on a Kinomica patent; LN—is an employee at Kinomica, owns Kinomica share options, Kinomica funded attendance and travel to conferences; SFP—is an employee at Kinomica, owns Kinomica share options; AEC—is an employee at Kinomica, owns Kinomica share options, Kinomica funded attendance and travel to conferences; NN—is an employee at Kinomica, owns Kinomica share options, Kinomica funded attendance and travel to conferences; JAC—is an employee at Kinomica, owns Kinomica share options, Kinomica funded attendance and travel to conferences; DNP—is an employee at Kinomica, owns Kinomica share options, Kinomica funded attendance and travel to conferences; PMC—is an employee at Kinomica, owns Kinomica share options, Kinomica funded attendance and travel to conferences; JK—is an employee at Kinomica, owns Kinomica share options; HRF—no conflict of interest; BP—no conflict of interest; PG—no conflict of interest; AA—no conflict of interest; AJA—received a honorarium for speaking engagements from Astellas; AT—received consultant fees from Kinomica for the role of Programme Director; AW—owns Kinomica share options, funded attendance and travel to conferences; GG—no conflict of interest; MDM—no conflict of interest; JGG—Kinomica co-founder, owns Kinomica share options; DJB—co-founder of Kinomica, owns Kinomica share options, named on Kinomica patents, Kinomica funded attendance and travel to conferences, received honoraria from Kinomica in a consulting role; PRC—co-founder and director of Kinomica, owns Kinomica share options, named on Kinomica patents, Kinomica funded attendance and travel to conferences, received honoraria from Kinomica in a consulting role; ADD—is an employee at Kinomica (CTO), named on Kinomica patents, Kinomica funded attendance and travel to conferences owns Kinomica share options.
Figures




References
-
- Shallis R.M., Wang R., Davidoff A., Ma X., Zeidan A.M. Epidemiology of acute myeloid leukemia: recent progress and enduring challenges. Blood Rev. 2019;36:70–87. - PubMed
-
- Döhner H., Wei A.H., Appelbaum F.R., et al. Diagnosis and management of AML in adults: 2022 recommendations from an international expert panel on behalf of the ELN. Blood. 2022;140(12):1345–1377. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
