

Single-cell AI-based detection and prognostic and predictive value of DNA mismatch repair deficiency in colorectal cancer
- PMID: 39293403
- PMCID: PMC11525017
- DOI: 10.1016/j.xcrm.2024.101727
Single-cell AI-based detection and prognostic and predictive value of DNA mismatch repair deficiency in colorectal cancer
Abstract
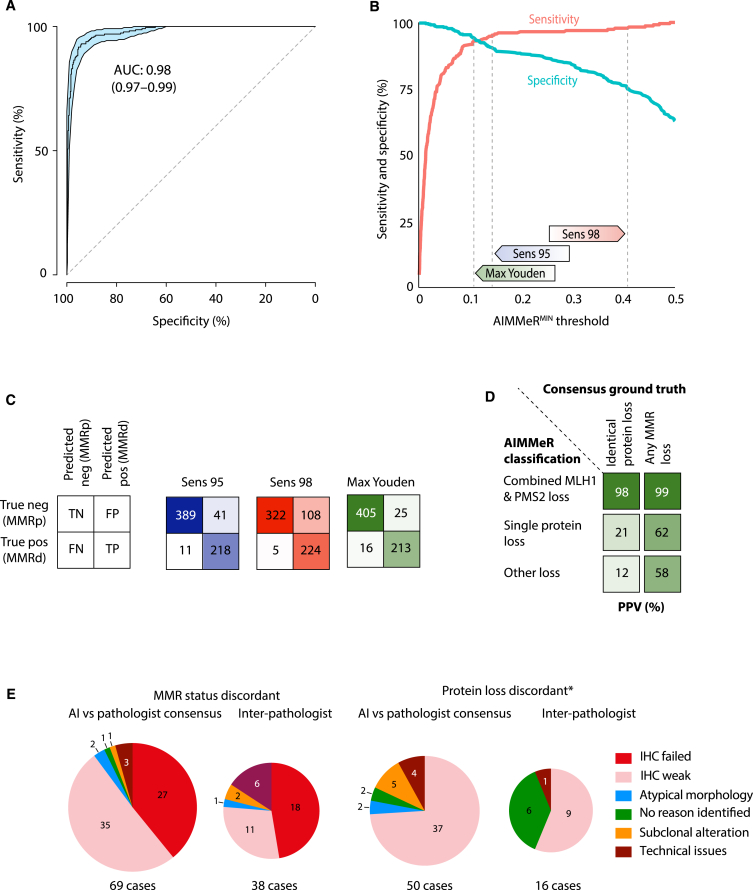
Testing for DNA mismatch repair deficiency (MMRd) is recommended for all colorectal cancers (CRCs). Automating this would enable precision medicine, particularly if providing information on etiology not captured by deep learning (DL) methods. We present AIMMeR, an AI-based method for determination of mismatch repair (MMR) protein expression at a single-cell level in routine pathology samples. AIMMeR shows an area under the receiver-operator curve (AUROC) of 0.98, and specificity of ≥75% at 98% sensitivity against pathologist ground truth in stage II/III in two trial cohorts, with positive predictive value of ≥98% for the commonest pattern of somatic MMRd. Lower agreement with microsatellite instability (MSI) testing (AUROC 0.86) reflects discordance between MMR and MSI PCR rather than AIMMeR misclassification. Analysis of the SCOT trial confirms MMRd prognostic value in oxaliplatin-treated patients; while MMRd does not predict differential benefit of chemotherapy duration, it correlates with difference in relapse by regimen (PInteraction = 0.04). AIMMeR may help reduce pathologist workload and streamline diagnostics in CRC.
Keywords: AI; colorectal cancer; digital pathology; microsatellite instability; mismatch repair deficiency.
Copyright © 2024 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests D.N.C. has participated in advisory boards for MSD and has received research funding on behalf of the TransSCOT consortium from HalioDx for analyses independent of this study. V.H.K. has served as an invited speaker on behalf of Indica Labs, SPCC, and Takeda and has received project-based research funding from The Image Analysis Group and Roche outside of the submitted work.
Figures





References
-
- Haraldsdottir S., Hampel H., Tomsic J., Frankel W.L., Pearlman R., de la Chapelle A., Pritchard C.C. Colon and Endometrial Cancers with Mismatch Repair Deficiency can Arise from Somatic, Rather Than Germline, Mutations. Gastroenterology. 2014;147:1308–1316.e1. doi: 10.1053/j.gastro.2014.08.041. - DOI - PMC - PubMed
-
- Mensenkamp A.R., Vogelaar I.P., van Zelst-Stams W.A., Goossens M., Ouchene H., Hendriks-Cornelissen S.J., Kwint M.P., Hoogerbrugge N., Nagtegaal I.D., Ligtenberg M.J. Somatic mutations in MLH1 and MSH2 are a frequent cause of mismatch-repair deficiency in Lynch syndrome-like tumors. Gastroenterology. 2014;146:643–646.e648. doi: 10.1053/j.gastro.2013.12.002. - DOI - PubMed
-
- Kane M.F., Loda M., Gaida G.M., Lipman J., Mishra R., Goldman H., Jessup J.M., Kolodner R. Methylation of the hMLH1 promoter correlates with lack of expression of hMLH1 in sporadic colon tumors and mismatch repair-defective human tumor cell lines. Cancer Res. 1997;57:808–811. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
