

Neutrophil serine proteases in cystic fibrosis: role in disease pathogenesis and rationale as a therapeutic target
- PMID: 39293854
- PMCID: PMC11409056
- DOI: 10.1183/16000617.0001-2024
Neutrophil serine proteases in cystic fibrosis: role in disease pathogenesis and rationale as a therapeutic target
Abstract
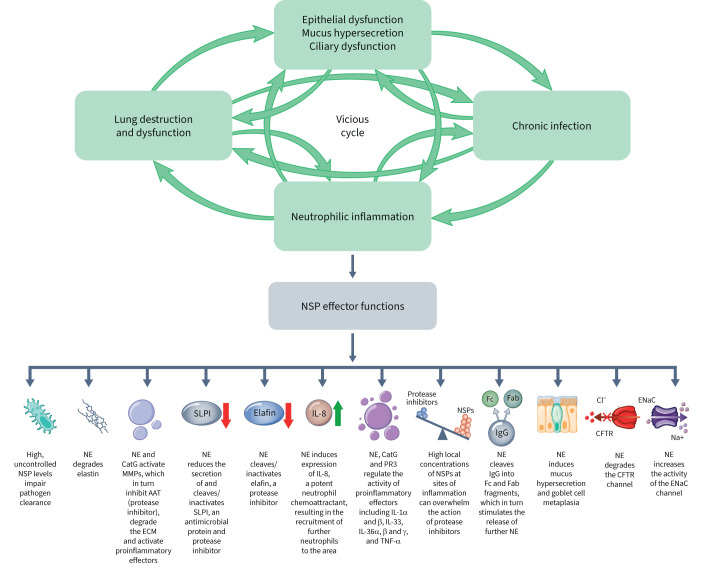
Chronic airway inflammation is a central feature in the pathogenesis of bronchiectasis (BE), which can be caused by cystic fibrosis (CFBE; hereafter referred to as CF lung disease) and non-CF-related conditions (NCFBE). Inflammation in both CF lung disease and NCFBE is predominantly driven by neutrophils, which release proinflammatory cytokines and granule proteins, including neutrophil serine proteases (NSPs). NSPs include neutrophil elastase, proteinase 3 and cathepsin G. An imbalance between NSPs and their antiproteases has been observed in people with CF lung disease and people with NCFBE. While the role of the protease/antiprotease imbalance is well established in both CF lung disease and NCFBE, effective therapies targeting NSPs are lacking. In recent years, the introduction of CF transmembrane conductance regulator (CFTR) modulator therapy has immensely improved outcomes in many people with CF (pwCF). Despite this, evidence suggests that airway inflammation persists, even in pwCF treated with CFTR modulator therapy. In this review, we summarise current data on neutrophilic inflammation in CF lung disease to assess whether neutrophilic inflammation and high, uncontrolled NSP levels play similar roles in CF lung disease and in NCFBE. We discuss similarities between the neutrophilic inflammatory profiles of people with CF lung disease and NCFBE, potentially supporting a similar therapeutic approach. Additionally, we present evidence suggesting that neutrophilic inflammation persists in pwCF treated with CFTR modulator therapy, at levels similar to those in people with NCFBE. Collectively, these findings highlight the ongoing need for new treatment strategies targeting neutrophilic inflammation in CF lung disease.
Copyright ©The authors 2024.
Conflict of interest statement
Conflict of interest: M.A. Mall has received research grants paid to their institution from the German Research Foundation (DFG), German Ministry for Education and Research (BMBF), German Innovation Fund and Vertex Pharmaceuticals; consultancy fees from Abbvie, Antabio, Arrowhead, Boehringer Ingelheim, Enterprise Therapeutics, Kither Biotec, Prieris, Recode, Santhera, Splisense and Vertex Pharmaceuticals; speaker fees from Vertex Pharmaceuticals; and travel grants for participation in advisory boards for Boehringer Ingelheim and Vertex Pharmaceuticals. M.A. Mall is listed as inventor on an issued patent filed by the University of North Carolina at Chapel Hill, describing the Scnn1b-transgenic mouse. M.A. Mall also reports advisory board participation for Abbvie, Antabio, Arrowhead, Boehringer Ingelheim, Enterprise Therapeutics, Kither Biotec, Pari and Vertex Pharmaceuticals, and is a fellow of ERS. J.C. Davies has received research grants from the UK Cystic Fibrosis Trust, Cystic Fibrosis Foundation, Cystic Fibrosis Ireland, EPSRC and NIHR, has received fees for clinical trial leadership and/or advisory board participation and speaking roles from Abbvie, Algipharma, Arcturus, Boehringer Ingelheim, Eloxx, Enterprise Therapeutics, Genentech, LifeArc, Recode, Tavanta and Vertex Pharmaceuticals, and is the Deputy Editor for the Journal of Cystic Fibrosis. J.C. Davies acknowledges funding from the National Institute of Health and Care Research through the Imperial Biomedical Research Centre and a Senior Investigator Award and grant funding from the Cystic Fibrosis Trust. S.H. Donaldson reports grants from the Cystic Fibrosis Foundation and the NIH; clinical trial contracts from AstraZeneca, Calithera and Vertex Pharmaceuticals; consulting fees from Chiesi USA, Inc., Polarean and 501 Ventures; and travel grants from Enterprise Therapeutics and Gilead Sciences. S.H. Donaldson also reported advisory board participation for Boehringer Ingelheim and data and safety monitoring board participation for Abbvie. R. Jain reports research grants from the CF Foundation, consulting fees from Boehringer Ingelheim, Insmed and Recode, and payment of honoraria for participation in the Vertex Innovation Awards review committee from Vertex Pharmaceuticals. R. Jain also reports advisory/data and safety monitoring board participation for Armata. J.D. Chalmers has received research grants from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Gilead Sciences, Grifols, Novartis, Insmed and Zambon, and has received consultancy fees from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Insmed, Pfizer and Zambon. M. Shteinberg reports having received research grants paid to their institution from GlaxoSmithKline, Novartis and Trudell; travel grants from Actelion, Boehringer Ingelheim, GlaxoSmithKline, Novartis, and Rafa; speaker fees from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Kamada, Novartis, Sanofi and Teva; and consultancy fees from Boehringer Ingelheim, GlaxoSmithKline, Kamada and Zambon. M. Shteinberg also reports data and safety monitoring board participation for Bonus Therapeutics, Israel and has unpaid roles in EMBARC, the Israel Pulmonology Society board and the Israel Society for TB and Mycobacterial Diseases.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical