

Targeted proteomics of cerebrospinal fluid in treatment naïve multiple sclerosis patients identifies immune biomarkers of clinical phenotypes
- PMID: 39294186
- PMCID: PMC11411093
- DOI: 10.1038/s41598-024-67769-1
Targeted proteomics of cerebrospinal fluid in treatment naïve multiple sclerosis patients identifies immune biomarkers of clinical phenotypes
Abstract
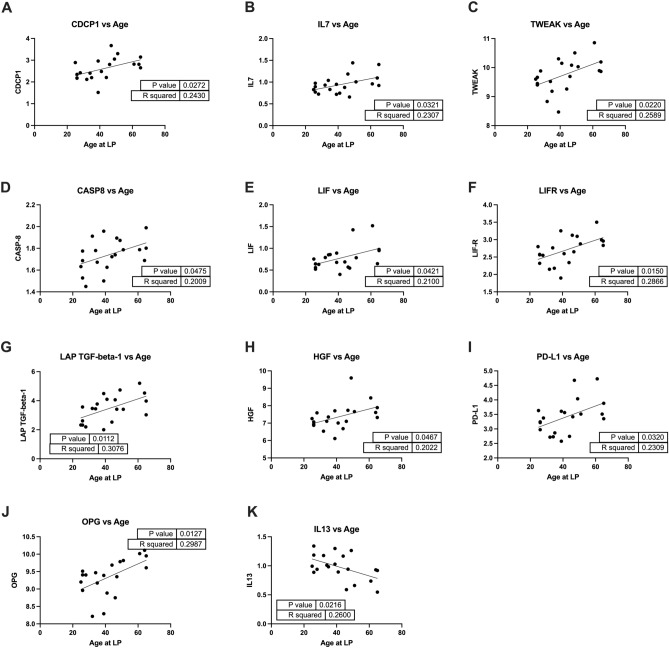
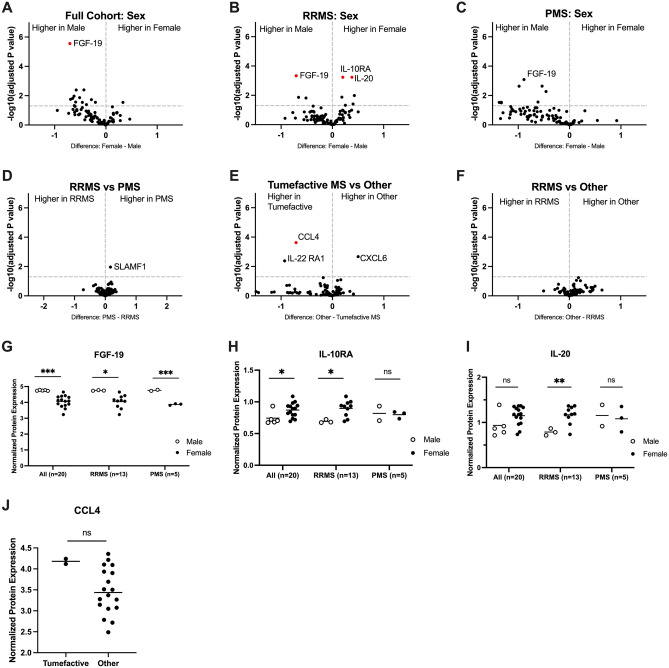
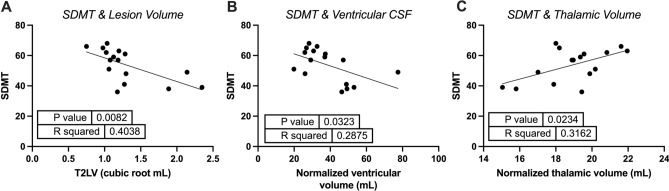
Multiple sclerosis (MS) is an inflammatory demyelinating disease with heterogeneous clinical presentations and variable long-term disability accumulation. There are currently no standard criteria to accurately predict disease outcomes. In this study we investigated the cross-sectional relationship between disease phenotype and immune-modulating cytokines and chemokines in cerebrospinal fluid (CSF). We analyzed CSF from 20 DMT-naïve MS patients using Olink Proteomics' Target 96 Inflammation panel and correlated the resulting analytes with respect to (1) disease subtype, (2) patient age and sex, (3) extent of clinical disability, and (4) MRI segmental brain volumes. We found that intrathecal IL-4 correlated with higher Expanded Disability Status Scale (EDSS) scores and longer 25-foot walk times, and CD8A correlated with decreased thalamic volumes and longer 9-hole peg test times. Male sex was associated with higher FGF-19 expression, and Tumefactive MS with elevated CCL4. Several inflammatory markers were correlated with older age at the time of LP. Finally, higher intrathecal IL-33 correlated with increased MS lesion burden and multi-compartment brain atrophy. This study confirms immune heterogeneity underlying CSF profiles in MS, but also identifies several inflammatory protein biomarkers that may be of use for predicting clinical outcomes in future algorithms.
Keywords: Age; Cerebrospinal fluid (CSF); Expanded Disability Status Scale (EDSS); Multiple sclerosis (MS); Targeted proteomics.
© 2024. The Author(s).
Conflict of interest statement
JMR is an inventor on patent application #15/851,651, “Anti111-human CXCR3 antibodies for the Treatment of Vitiligo” which covers targeting CXCR3 for the treatment of vitiligo; and on patent #62489191, “Diagnosis and Treatment of Vitiligo” which covers targeting IL-15 and Trm for the treatment of vitiligo. The remaining authors declare that the research was conducted in the absence of any competing interests that could be construed as a potential conflict of interest.
Figures


References
-
- Dobson, R. & Giovannoni, G. Multiple sclerosis—A review. Eur. J. Neurol.26, 27–40. 10.1111/ene.13819 (2019). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
