

Frequent CHD1 deletions in prostate cancers of African American men is associated with rapid disease progression
- PMID: 39294262
- PMCID: PMC11411125
- DOI: 10.1038/s41698-024-00705-8
Frequent CHD1 deletions in prostate cancers of African American men is associated with rapid disease progression
Abstract
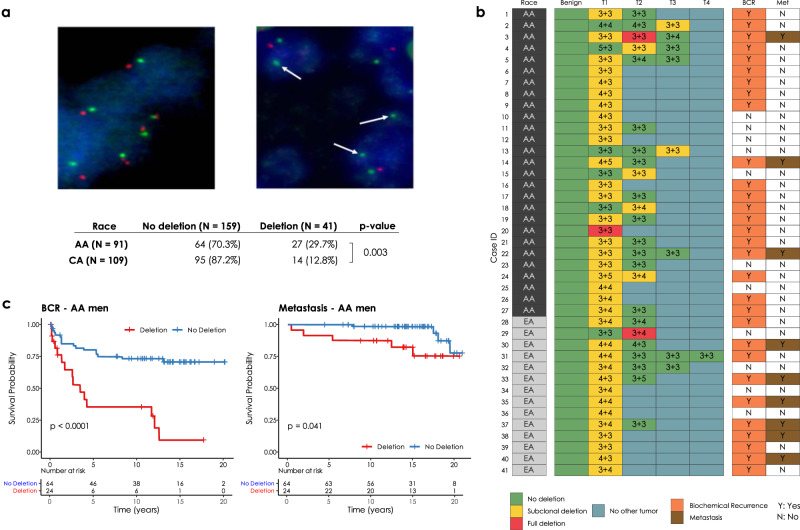
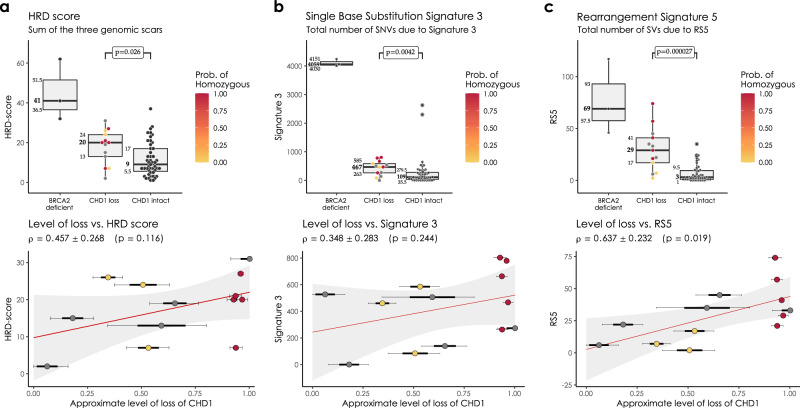
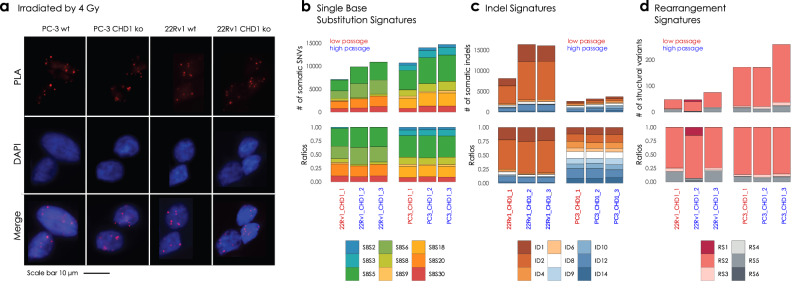
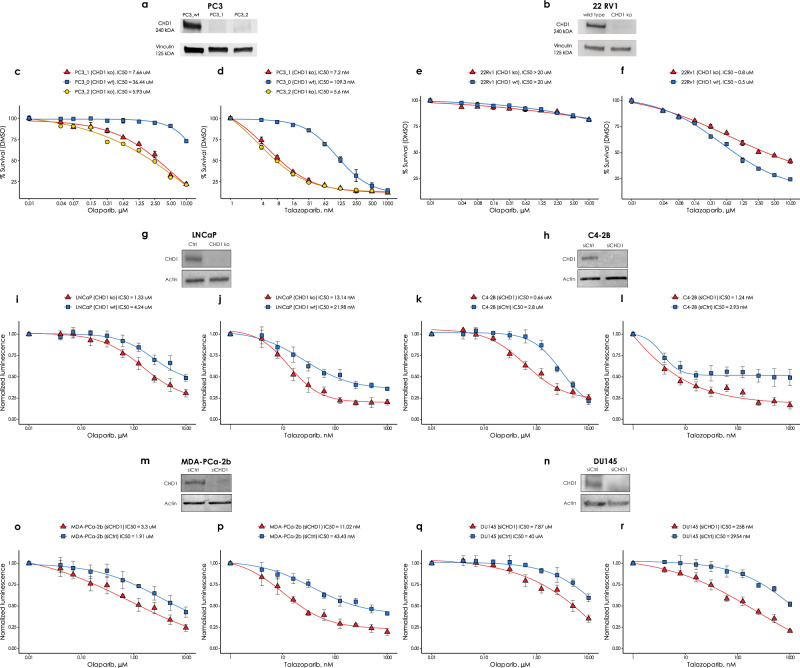
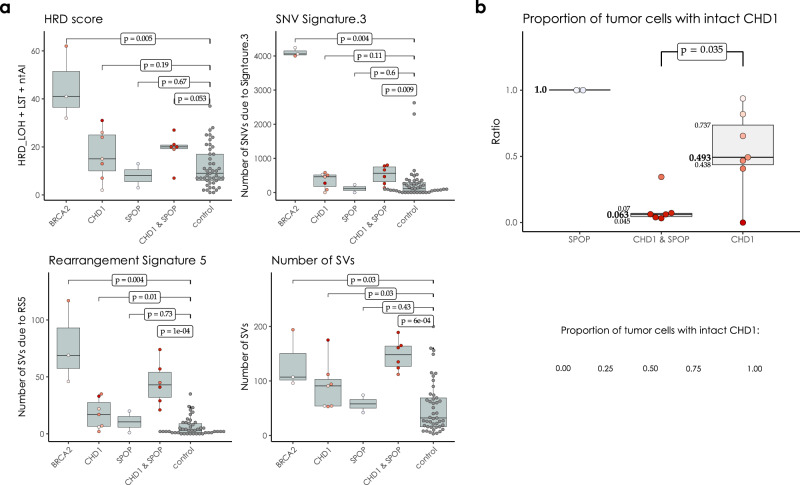
We analyzed genomic data from the prostate cancer of African- and European American men to identify differences contributing to racial disparity of outcome. We also performed FISH-based studies of Chromodomain helicase DNA-binding protein 1 (CHD1) loss on prostate cancer tissue microarrays. We created CHD1-deficient prostate cancer cell lines for genomic, drug sensitivity and functional homologous recombination (HR) activity analysis. Subclonal deletion of CHD1 was nearly three times as frequent in prostate tumors of African American than in European American men and it associates with rapid disease progression. CHD1 deletion was not associated with HR deficiency associated mutational signatures or HR deficiency as detected by RAD51 foci formation. This was consistent with the moderate increase of olaparib and talazoparib sensitivity with several CHD1 deficient cell lines showing talazoparib sensitivity in the clinically relevant concentration range. CHD1 loss may contribute to worse disease outcome in African American men.
© 2024. The Author(s).
Conflict of interest statement
Z. Szallasi is listed as a co-inventor on a patent to quantify homologous recombination deficiency, which is owned by Children’s Hospital Boston and licensed to Myriad Genetics. No potential conflicts of interest were disclosed by the other authors.
Figures
Update of
-
Increased frequency of CHD1 deletions in prostate cancers of African American men is associated with rapid disease progression without inducing homologous recombination deficiency.Res Sq [Preprint]. 2024 Apr 1:rs.3.rs-3995251. doi: 10.21203/rs.3.rs-3995251/v1. Res Sq. 2024. Update in: NPJ Precis Oncol. 2024 Sep 19;8(1):208. doi: 10.1038/s41698-024-00705-8. PMID: 38645014 Free PMC article. Updated. Preprint.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
