

[18F]FDG-PET/CT in adrenal lesions: diagnostic performance in different clinical settings
- PMID: 39294519
- PMCID: PMC11739187
- DOI: 10.1007/s12020-024-04042-5
[18F]FDG-PET/CT in adrenal lesions: diagnostic performance in different clinical settings
Abstract
Purpose: Data regarding [18F]FDG-PET/CT for the characterization of adrenal lesions are limited. Most of the studies proposed the tumor-to-liver maximum standardized uptake values (SUVratio) > 1.5 as the best cut off to predict malignancy. The aim of the study was to calculate the optimum cut off in a heterogeneous population with adrenal lesions and evaluate the diagnostic performance SUVratio >1.5.
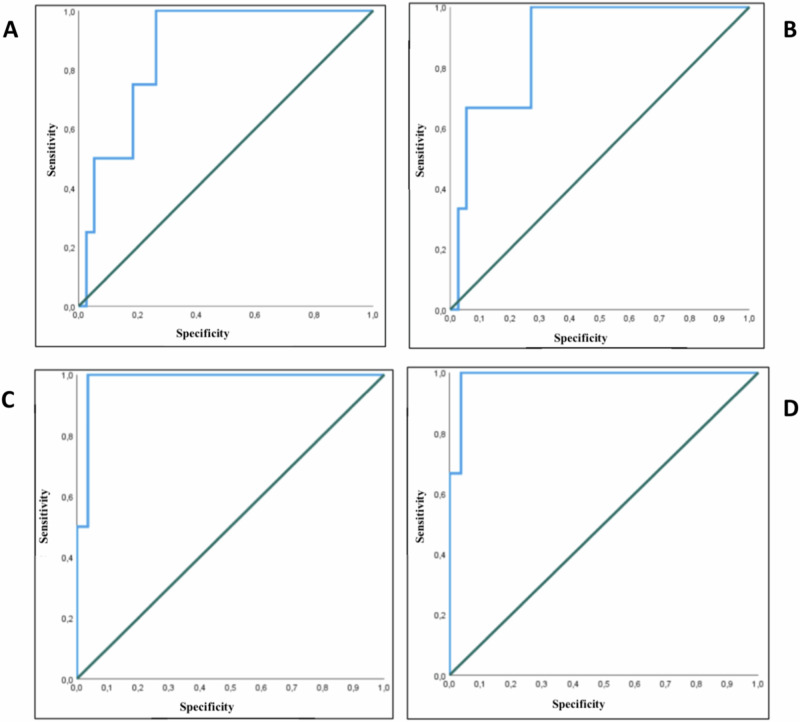
Patients and methods: Retrospective analysis of adrenal lesions undergoing [18F]FDG-PET/CT (2013-2022) for different reasons (atypical adrenal incidentalomas, extra adrenal tumor staging). The diagnosis of benignity was assessed by: (i) histology; (ii) stability or minimal diameter increase (<20%/<5 mm) on 12-months follow-up for non-operated patients. The optimal SUVratio and performance of SUVratio >1.5 were calculated by ROC curves.
Results: Forty-two consecutive lesions (diameter 36.1 ± 20.3 mm, 6 bilateral) underwent [18F]FDG-PET/CT (19F, age 61.2 ± 11.7 years). Twenty-nine lesions were benign, 11 malignant [8 metastases (2 bilateral) and 1 adrenocortical carcinoma (ACC)] and 2 pheochromocytomas. The SUVratio cut-off in our population was 1.55 (Sn 100%, Sp 73.7%, AUC 0.868), with similar values excluding pheochromocytomas and metastases (SUVratio cut-off 1.49, Sn 100%, Sp 96.3%, AUC 0.988). The SUVratio cut-off of 1.5 showed 100% Sn, 87% Sp, 73% PPV, and 100% NPV.
Conclusion: [18F]FDG-PET/CT could help in decision making process avoiding unnecessary surgery. The SUVratio cut-off of 1.5 has a good performance in a heterogenous population.
Keywords: Adrenal; SUV ratio; Sensitivity; Specificity; [18F]FDG-PET/CT.
© 2024. The Author(s).
Conflict of interest statement
Compliance with ethical standards. Conflict of interest: The authors declare no competing interests.
Figures
References
-
- C. Guerin, F. Pattou, L. Brunaud, J.C. Lifante, E. Mirallié, M. Haissaguerre, D. Huglo, P. Olivier, C. Houzard, C. Ansquer, E. Hindié, A. Loundou, C. Archange, A. Tabarin, F. Sebag, K. Baumstarck, D. Taïeb, Performance of 18F-FDG PET/CT in the characterization of adrenal masses in noncancer patients: a prospective study. J. Clin. Endocrinol. Metab. 102, 2465–2472 (2017). 10.1210/jc.2017-00254 - PubMed
-
- M.M. Grumbach, B.M. Biller, G.D. Braunstein, K.K. Campbell, J.A. Carney, P.A. Godley, E.L. Harris, J.K. Lee, Y.C. Oertel, M.C. Posner, J.A. Schlechte, H.S. Wieand, Management of the clinically inapparent adrenal mass (incidentaloma). Ann. Intern. Med. 138, 424–429 (2003). 10.7326/0003-4819-138-5-200303040-00013 - PubMed
-
- R.T. Kloos, M.D. Gross, I.R. Francis, M. Korobkin, B. Shapiro, Incidentally discovered adrenal masses. Endocr. Rev. 16, 460–484 (1995). 10.1210/edrv-16-4-460 - PubMed
-
- G. Mansmann, J. Lau, E. Balk, M. Rothberg, Y. Miyachi, S.R. Bornstein, The clinically inapparent adrenal mass: update in diagnosis and management. Endocr. Rev. 25, 309–340 (2004). 10.1210/er.2002-0031 - PubMed
-
- L. Barzon, N. Sonino, F. Fallo, G. Palu, M. Boscaro, Prevalence and natural history of adrenal incidentalomas. Eur. J. Endocrinol. 149, 273–285 (2003). 10.1530/eje.0.1490273 - PubMed
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
