

Haemodynamic effects of intra-aortic balloon pumps stratified by baseline pulmonary artery pulsatility index
- PMID: 39294848
- PMCID: PMC11769640
- DOI: 10.1002/ehf2.15083
Haemodynamic effects of intra-aortic balloon pumps stratified by baseline pulmonary artery pulsatility index
Abstract
Aims: Intra-aortic balloon pump (IABP) devices are commonly used in patients with heart failure related cardiogenic shock (HF-CS), including those with out-of-proportion right ventricular (RV) dysfunction. Pulmonary artery pulsatility index (PAPi) is a haemodynamic surrogate for RV performance. We aimed to assess short-term haemodynamic changes in patients with HF-CS following IABP support stratified by baseline PAPi.
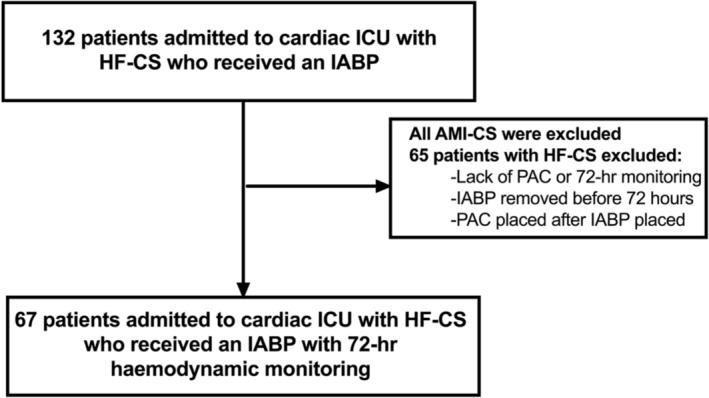
Methods and results: This is a single-centre study of 67 consecutive patients with HF-CS who underwent IABP placement between 2020 and 2022. The primary aim was haemodynamic changes of specific variables on pulmonary artery catheter monitoring over 72 h following IABP placement. Secondary aims were clinically significant changes in diuretic regimens, changes in inotropes or vasopressors at 72 h following IABP, along with clinical outcomes. Prior to IABP placement, 57% of the total cohort (median age 59 years [48, 69], 31% female) had Society of Cardiovascular Angiography and Interventions Stage C HF-CS. Thirty-eight (56%) patients had a PAPi <2.0. Following 72 h of IABP support, the PAPi <2.0 group had an observed significant decrease in central venous pressure (CVP; 20 to 12 mmHg, P < 0.001) and mean pulmonary artery pressure (mPAP; 37.5 to 28.5 mmHg, P = 0.001), and an increase in PAPi (1 to 1.6, P = 0.001). No significant change in cardiac index (CI; 2 to 2.1 L/min/m2, P = 0.31) was observed. The PAPi ≥2.0 group (N = 29) had no observed significant change in CVP (10 to 8 mmHg, P = 0.47), or PAPi (2.6 to 2.8, P = 0.92), but there was a significant improvement in CI (1.9 to 2.5 L/min/m2, P = 0.004) along with reduction in mPA (37 to 29 mmHg, P = 0.03). The PAPi <2.0 group had a significant increase in diuretic requirement (52.6% vs. 20.7%, P = 0.01) and numerically greater addition of inotropes/vasopressors (47.3% vs. 34.4%, P = 0.07) compared with the PAPi ≥2.0 group at 72 h following IABP placement. Significantly more patients in the PAPi ≥2.0 group underwent left ventricular assist device (55.2% vs. 26.3%, P = 0.02), with no overall significant differences observed in escalation to veno-arterial extracorporeal membrane oxygenation, 30-day mortality, renal replacement therapy post-IABP, or rates of heart transplantation.
Conclusions: IABP devices in those with HF-CS and low or abnormal PAPi may provide modest short-term haemodynamic benefits without significant improvement in CI, along with greater need for adjustment in medical therapeutics to achieve haemodynamic optimization.
Keywords: Cardiogenic shock; Haemodynamics; Mechanical circulatory support.
© 2024 The Author(s). ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
N.N. received speaker fees from Boehringer Ingelheim and AztraZeneca. S.P. received speaker fees from AztraZeneca. G.M. received speaker fees from Lexicon Pharmaceuticals and AztraZeneca. No industry relationships have directly impacted the work of this manuscript. All other authors have no disclosures.
Figures



References
-
- Geller BJ, Sinha SS, Kapur NK, Bakitas M, Balsam LB, Chikwe J, et al. Escalating and de‐escalating temporary mechanical circulatory support in cardiogenic shock: a scientific statement from the American Heart Association. Circulation 2022;146:e50‐e68. doi: 10.1161/CIR.0000000000001076 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
