

The immune response to Covid-19 mRNA vaccination among Lymphoma patients receiving anti-CD20 treatment
- PMID: 39295862
- PMCID: PMC11408186
- DOI: 10.3389/fimmu.2024.1433442
The immune response to Covid-19 mRNA vaccination among Lymphoma patients receiving anti-CD20 treatment
Abstract
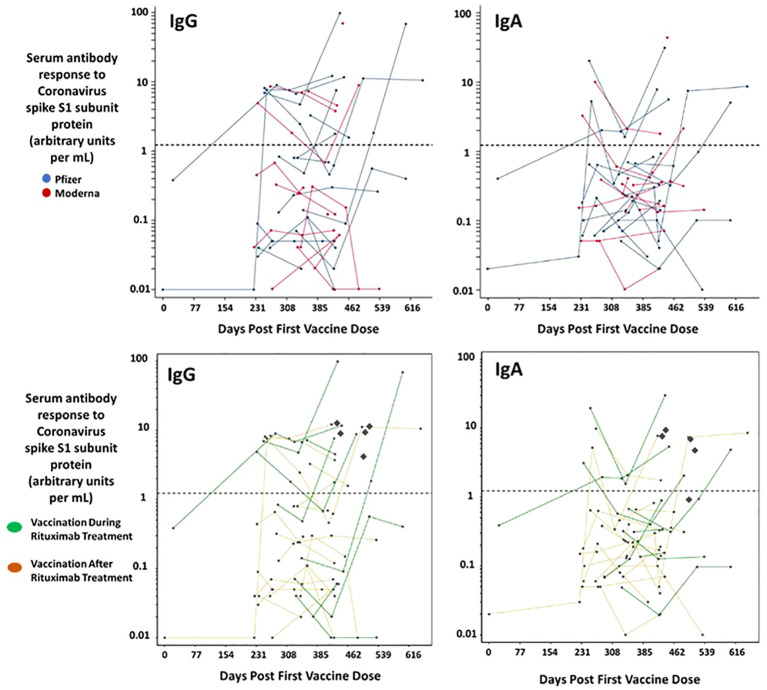
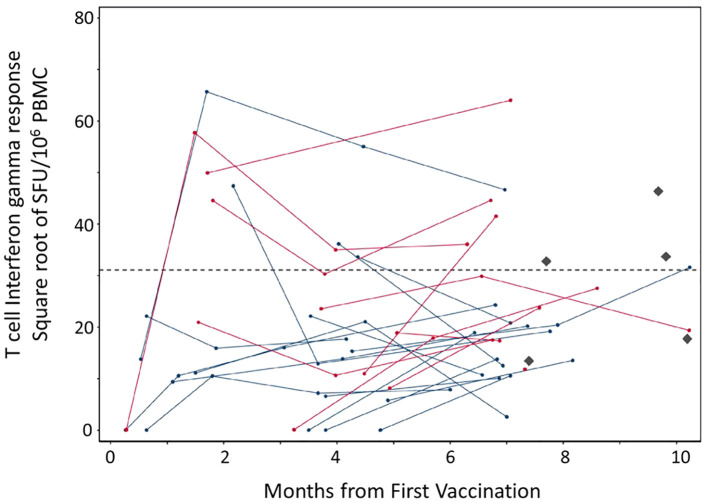
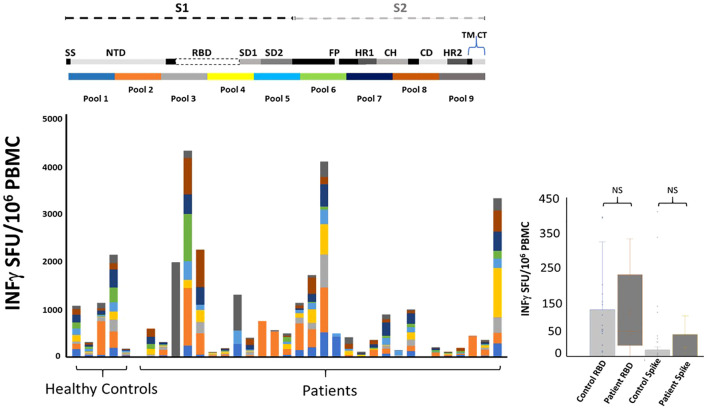
The monoclonal antibody rituximab improves clinical outcome in the treatment of CD20-positive lymphomatous neoplasms, and it is an established drug for treatment of these cancers. Successful mRNA COVID-19 (SARS-CoV-2) vaccination is extremely important for lymphoma patients because they tend to be elderly with comorbidities which leaves them at increased risk of poor outcomes once infected by Coronavirus. Anti-CD20 therapies such as rituximab, deplete B-cell populations and can affect vaccine efficacy. Therefore, a knowledge of the effect of COVID-19 vaccination in this group is critical. We followed a cohort of 28 patients with CD20-positive lymphomatous malignancies treated with rituximab that started prior to their course of COVID-19 vaccination, including boosters. We assayed for vaccine "take" in the humoral (IgG and IgA) and cellular compartment. Here, we show that short-term and long-term development of IgG and IgA antibodies directed toward COVID-19 spike protein are reduced in these patients compared to healthy controls. Conversely, the robustness and breath of underlying T-cell response is equal to healthy controls. This response is not limited to specific parts of the spike protein but spans the spike region, including response to the conserved Receptor Binding Domain (RBD). Our data informs on rational vaccine design and bodes well for future vaccination strategies that require strong induction of T-cell responses in these patients.
Keywords: CD20; COVID - 19; Tcell; lymphoma; mRNA; rituximab; vaccination.
Copyright © 2024 Komlodi-Pasztor, Escarra-Senmarti, Bazer, Bhatnagar, Perez Heydrich, Messmer, Ambinder, Gladstone, Clayton, Goodrich, Schoch, Wagner-Johnston, VandenBussche, Huang, Holdhoff and Rosario.
Conflict of interest statement
MH: Advisory Board: Servier, Novartis, AnHeart, Bayer; Steering Committee: Novartis; Honoraria for educational talks: Pfizer (educational talk for Pfizer staff in 2021), Novartis; Data Safety Monitoring Board: Advarra, Parexel. MR: Patent applications have been filed and are currently pending in US, US-2023-0372469, and Europe, EP 4228686 for a T cell vaccine for SARS virus. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Kroger A, Bahta L, Long S, Sanchez P. ACIP altered immunocompetence guidelines for immunizations. Centers for Disease Control and Prevention (2023). Available online at: https://www.cdc.gov/vaccines/hcp/acip-recs/general-recs/immunocompetence....
-
- McLaughlin P, Grillo-López AJ, Link BK, Levy R, Czuczman MS, Williams ME, et al. Rituximab chimeric anti-CD20 monoclonal antibody therapy for relapsed indolent lymphoma: half of patients respond to a four-dose treatment program. J Clin Oncol. (1998) 16:2825–33. doi: 10.1200/JCO.1998.16.8.2825 - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous