

Case report: Concurrent MOG antibody-associated disease and latent infections in two patients
- PMID: 39295869
- PMCID: PMC11408232
- DOI: 10.3389/fimmu.2024.1455355
Case report: Concurrent MOG antibody-associated disease and latent infections in two patients
Abstract
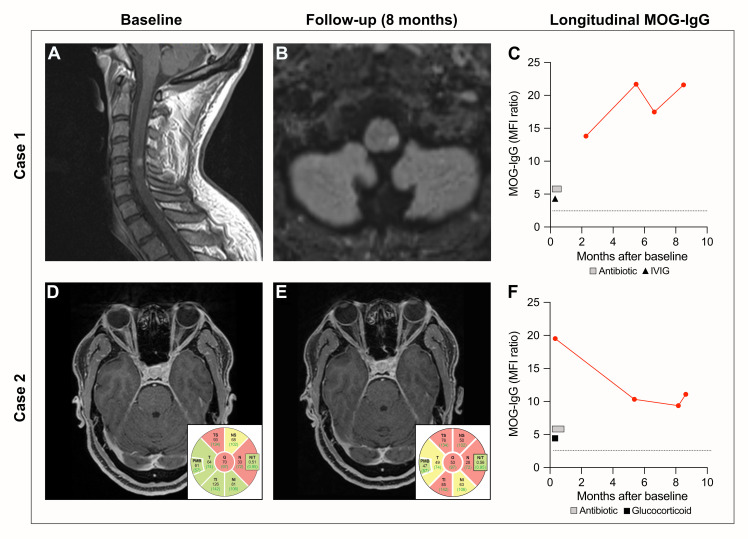
Objectives: Myelin oligodendrocyte glycoprotein (MOG) antibody-associated disease (MOGAD) is frequently preceded by infections. The underlying pathomechanism, however, remains poorly understood. Here, we present the clinical data of two MOGAD patients with concurrent syphilis infection and investigate the reactivity of patient-derived antibodies to MOG and Treponema pallidum (T. pallidum).
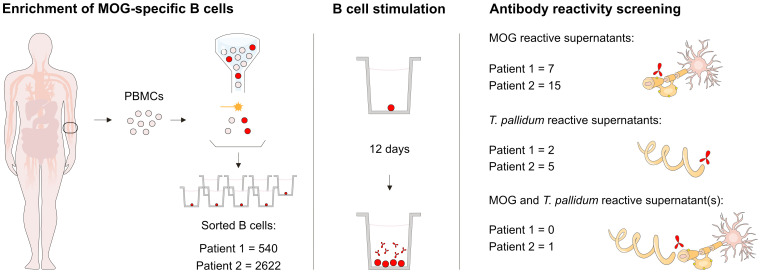
Methods: Longitudinal serum samples and soluble immunoglobulins in single B cell supernatants were measured for MOG reactivity by a live cell-based assay. Reactivity against T. pallidum was assessed by enzyme-linked immunosorbent assay.
Results: The two patients presented MOGAD and concurrent latent syphilis infection, manifesting as cervical myelitis and unilateral optic neuritis, respectively. The first patient had been living with HIV on antiretroviral therapy, and the second was concomitantly diagnosed with chronic hepatitis B infection. Upon screening of B cell supernatants, we identified reactivity to MOG or T. pallidum. Notably, one B cell showed reactivity to both antigens.
Discussion: The coexistence of MOGAD diagnoses and latent syphilis, alongside the identification of antibody reactivity to MOG and T. pallidum, underscores the potential pathomechanistic link between syphilis infection and subsequent autoimmune neuroinflammation. Cross-reactivity between MOG and T. pallidum antibodies remains to be validated on a molecular level, and further characterization of infectious triggers associated with MOGAD is needed.
Keywords: B cells; antibodies; case report; infection; molecular mimicry; myelin oligodendrocyte glycoprotein; myelin oligodendrocyte glycoprotein antibody-associated disease; syphilis.
Copyright © 2024 Kulsvehagen, Woelfle, Ayroza Galvão Ribeiro Gomes, Lipps, Neziraj, Flammer, Leuzinger, Derfuss, Kuhle, Papadopoulou and Pröbstel.
Conflict of interest statement
AA has received a research grant from Roche and travel grants from Roche and Biogen. JK received speaker fees, research support, and travel support and/or served on advisory boards by the Swiss MS Society, Swiss National Research Foundation 320030_189140/1, University of Basel, Progressive MS Alliance, Bayer, Biogen, Bristol Myers Squibb, Celgene, Merck, Novartis, Octave Bioscience, Roche, and Sanofi. AP received financial compensation for participation in advisory boards and/or speaker fees from Eli Lilly, Lundbeck, Sanofi-Genzyme, and Teva, all used for research support; she also received travel support from Bayer AG, Eli Lilly, F. Hoffmann-La Roche, and Teva. A-KP received financial compensation for participation in advisory boards and consultations from Biogen, Roche, and Novartis, all used for research support. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Ayroza Galvão Ribeiro Gomes AB, Kulsvehagen L, Lipps P, Cagol A, Cerdá-Fuertes N, Neziraj T, et al. Immunoglobulin A antibodies against myelin oligodendrocyte glycoprotein in a subgroup of patients with central nervous system demyelination. JAMA Neurol. (2023) 80:989–95. doi: 10.1001/jamaneurol.2023.2523 - DOI - PMC - PubMed
-
- Jarius S, Ruprecht K, Kleiter I, Borisow N, Asgari N, Pitarokoili K, et al. MOG-IgG in NMO and related disorders: A multicenter study of 50 patients. Part 2: Epidemiology, clinical presentation, radiological and laboratory features, treatment responses, and long-term outcome. J Neuroinflamm. (2016) 13:280. doi: 10.1186/s12974-016-0718-0 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical