

When mycosis fungoides seems not to be within the spectrum of clinical and histopathological differential diagnoses
- PMID: 39295886
- PMCID: PMC11406214
- DOI: 10.4081/dr.2024.10008
When mycosis fungoides seems not to be within the spectrum of clinical and histopathological differential diagnoses
Abstract
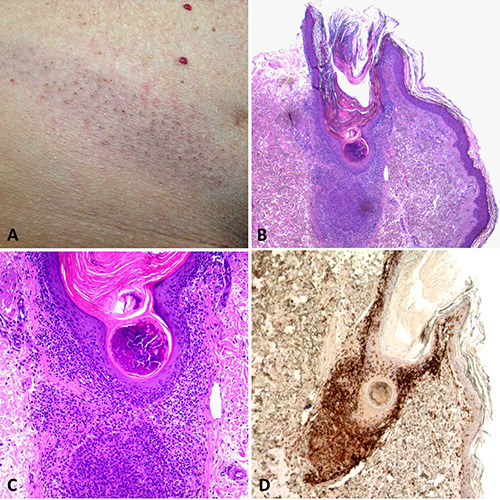
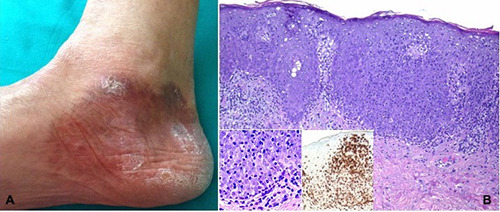
The most prevalent primary cutaneous T-cell lymphoma, mycosis fungoides (MF), is characterized by the development of plaques and nodules after an erythematous patchy phase that is non-specific. An infiltrate of atypical small- to medium-sized cerebriform lymphocytes in the superficial dermis, with variable epidermotropism, is the histopathological hallmark of the disease. In more advanced stages of the illness, large-cell transformation may be seen. Early diagnosis of MF can be very challenging based only on histopathologic or clinical findings, so it is critical to have a clinical-pathological correlation. Many atypical variants of MF that deviate from the classic Alibert-Bazin presentation of the disease have been described over the past 30 years, sometimes with different prognostic and therapeutic implications. Clinically or histopathologically, they can mimic a wide range of benign inflammatory skin disorders. To make a conclusive diagnosis in these cases, it is recommended to take multiple biopsies from various lesions and to carefully correlate the clinical and pathological findings. We have outlined the various facets of the illness in this review, positioning MF as a "great imitator", with an emphasis on the more recently identified variations, differential diagnosis, and its benign mimics.
Keywords: dermatopathology; mimickers; mycosis fungoides.
Copyright © 2024, the Author(s).
Conflict of interest statement
Conflict of interest: the authors declare no potential conflict of interest.
Figures












References
-
- Elder DE, Massi D, Scolyer RA WR. WHO Classification of Skin Tumours. 4th Edition. IARC Press; 2018.
-
- Muñoz-González H, Molina-Ruiz AM, Requena L. Clinicopathologic variants of mycosis fungoides. Actas Dermo-Sifiliográficas 2017;108:192-208. - PubMed
-
- Fauconneau A, Pham-Ledard A, Cappellen D, et al. Assessment of diagnostic criteria between primary cutaneous anaplastic large-cell lymphoma and CD30-rich transformed mycosis fungoides; A study of 66 cases. Br J Dermatol 2015;172:1547-54. - PubMed
-
- Massone C, Kodama K, Kerl H, Cerroni L. Histopathologic features of early (patch) lesions of mycosis fungoides: A morphologic study on 745 biopsy specimens from 427 patients. Am J Surg Pathol 2005;29:550-60. - PubMed
-
- Massone C, Crisman G, Kerl H, Cerroni L. The prognosis of early mycosis fungoides is not influenced by phenotype and T-cell clonality. Br J Dermatol 2008;159:881-6. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
