

Predicting Psoriatic Arthritis in Psoriasis Patients - A Swiss Registry Study
- PMID: 39295895
- PMCID: PMC11361495
- DOI: 10.1177/24755303231217492
Predicting Psoriatic Arthritis in Psoriasis Patients - A Swiss Registry Study
Abstract
Background: Psoriatic arthritis (PsA) is a prevalent comorbidity among patients with psoriasis, heavily contributing to their burden of disease, usually diagnosed several years after the diagnosis of psoriasis.
Objectives: To investigate the predictability of psoriatic arthritis in patients with psoriasis and to identify important predictors.
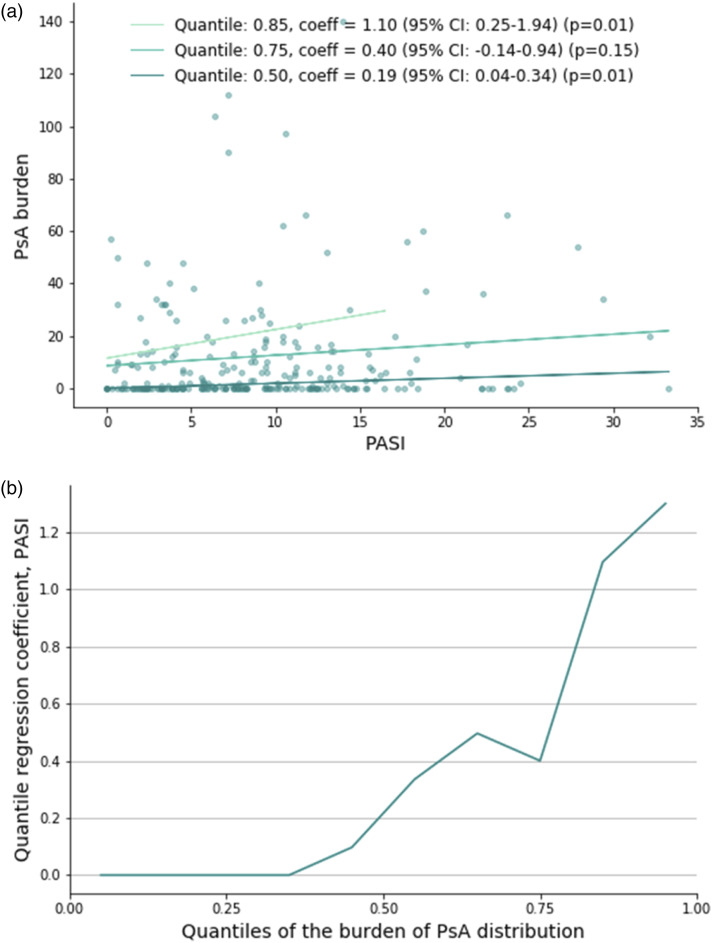
Methods: Data from the Swiss Dermatology Network on Targeted Therapies (SDNTT) involving patients treated for psoriasis were utilized. A combination of gradient-boosted decision trees and mixed models was used to classify patients based on their diagnosis of PsA or its absence. The variables with the highest predictive power were identified. Time to PsA diagnosis was visualized with the Kaplan-Meier method and the relationship between severity of psoriasis and PsA was explored through quantile regression.
Results: A diagnosis of psoriatic arthritis was registered at baseline of 407 (29.5%) treatment series. 516 patients had no registration of PsA, 257 patients had PsA at inclusion, and 91 patients were diagnosed with PsA after inclusion. The model's AUROCs was up to 73.7%, and variables with the highest discriminatory power were age, PASI, physical well-being, and severity of nail psoriasis. Among patients who developed PsA after inclusion, significantly more first treatment series were classified in the PsA-group, compared to those with no PsA registration. PASI was significantly correlated with the median burden/severity of PsA (P = .01).
Conclusions: Distinguishing between patients with and without PsA based on clinical characteristics is feasible and even predicting future diagnoses of PsA is possible. Patients at higher risk can be identified using important predictors of PsA.
Keywords: classification; machine learning; predictive models; psoriasis; psoriatic arthritis; real word; registry; statistics.
© The Author(s) 2023.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ms. Nielsen has nothing to declare Dr. Petersen has nothing to declare With no relation to the present manuscript Dr. LV Maul has served as advisor and/or received speaking fees and/or participated in clinical trials sponsored by Abbvie, Almirall, Amgen, Eli Lilly, MSD, Novartis, Pierre Fabre, Roche, and Sanofi. Dr. Thomsen has been a speaker or advisor for Sanofi, AbbVie, LEO Pharma, Pfizer, Eli Lilly, Novartis, UCB Pharma, Almirall, and Janssen Pharmaceuticals, and received research support from Sanofi, AbbVie, LEO Pharma, Novartis, UCB Pharma, and Janssen Pharmaceuticals, outside the submitted work. With no relation to the present manuscript, Dr. Schlapbach has received honoraria as adviser for Abbvie, BMS, LEO Pharma, Lilly, Kiowa Kirin, Novartis, and Pfizer and has received research funding from PPM Services. Prof. Kündig has intermittent, project focused consulting and/or advisory relationships with Leo Pharma, Janssen-Cilag, Eli Lilly, Pierre Fabre, Sanofi Genzyme, Abbvie, Biomed AG, Novartis, Almirall, Bristol-Myers Squibb, Galderma, L’Oréal/LaRoche-Posay, Merck-Sharp & Dohme, Zur Rose AG, Allergy Therapeutics AG, Derma2go AG, Oncobit AG, EVAX AG, Saiba Biotechnology AG, Saiba Animal Health AG, AltiBio Corp, Encoded Corp, Mabylon AG, MannKind Corp, XBiotech Corp. With no relation to the present manuscript, Dr. Wu is or has been an investigator, consultant, or speaker for AbbVie, Almirall, Amgen, Arcutis, Aristea Therapeutics, Bausch Health, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Codex Labs, Dermavant, DermTech, Dr. Reddy’s Laboratories, Eli Lilly, EPI Health, Galderma, Incyte, Janssen, LEO Pharma, Mindera, Novartis, Pfizer, Regeneron, Samsung Bioepis, Sanofi Genzyme, Solius, Sun Pharmaceutical, UCB, and Zerigo Health. Dr. Cozzio is or has been involved in advisory activities for AbbVie, Eli Lilly, Sanofi, Janssen-Cilag, Leo, Amgen. Dr. Conrad is or has been Scientific adviser and/or clinical study investigator for AbbVie, Actelion, Almirall, Amgen, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Eli-Lilly, Galderma, Incyte, Janssen, LEO pharma, MSD, Novartis, Pfizer, Samsung, Sanofi, and UCB With no relation to the present manuscript, Prof. Navarini declares being a consultant and advisor and/or receiving speaking fees and/or grants and/or served as an investigator in clinical trials for AbbVie, Almirall, Amgen, Biomed, BMS, Boehringer Ingelheim, Celgene, Eli Lilly, Galderma, GSK, LEO Pharma, Janssen-Cilag, MSD, Novartis, Pfizer, Pierre Fabre Pharma, Regeneron, Sandoz, Sanofi, and UCB. With no relation to the present manuscript Dr. Thyssen is a full time employee at LEO Pharma and is an advisor for AbbVie, Almirall, Arena Pharmaceuticals, Coloplast, OM Pharma, Aslan Pharmaceuticals, Union Therapeutics, Eli Lilly & Co, LEO Pharma, Pfizer, Regeneron, and Sanofi-Genzyme, a speaker for AbbVie, Almirall, Eli Lilly & Co, LEO Pharma, Pfizer, Regeneron, and Sanofi-Genzyme, and received research grants from Pfizer, Regeneron, and Sanofi-Genzyme. Dr. Boehncke has received honoraria as a speaker and/or advisor from Abbvie, Almirall, Amgen, BMS, Leo, Lilly, Novartis, and UCB. With no relation to the present manuscript Dr. Kristensen reports speakers bureau: Pfizer, AbbVie, Amgen, UCB, Galapagos, Biogen, BMS, MSD, Novartis, Eli Lilly, and Janssen pharmaceuticals & Consultancy for Pfizer, AbbVie, Amgen, UCB, Gilead, Biogen, BMS, MSD, Novartis, Eli Lilly, and Janssen pharmaceuticals. With no relation to the present manuscript Dr. Egeberg has received research funding from Pfizer, Eli Lilly, Novartis, Bristol-Myers Squibb, Boehringer Ingelheim, AbbVie, Janssen Pharmaceuticals, the Danish National Psoriasis Foundation, the Simon Spies Foundation, and the Kgl Hofbundtmager Aage Bang Foundation, and honoraria as consultant and/or speaker from AbbVie, Almirall, Leo Pharma, Zuellig Pharma Ltd., Galápagos NV, Sun Pharmaceuticals, Samsung Bioepis Co., Ltd., Pfizer, Eli Lilly and Company, Novartis, Galderma, Dermavant, UCB, Mylan, Bristol-Myers Squibb, McNeil Consumer Healthcare, Horizon Therapeutics, Boehringer Ingelheim, and Janssen Pharmaceuticals. With no relation to the present manuscript Dr. Maul has served as advisor and/or received speaking fees and/or participated in clinical trials sponsored by AbbVie, Almirall, Amgen, BMS, Celgene, Eli Lilly, LEO Pharma, Janssen-Cilag, MSD, Novartis, Pfizer, Pierre Fabre, Roche, Sanofi, UCB. With no relation to the present manuscript Dr. Yawalkar has served as advisor and/or received speaking fees and/or participated in clinical trials sponsored by AbbVie, Almirall, Amgen, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Eli Lilly, Galderma, LEO Pharma, Janssen-Cilag, MSD, Novartis, Pfizer, Sanofi-Genzyme, UCB.
Figures



References
-
- Alinaghi F, Calov M, Kristensen LE, et al. Prevalence of psoriatic arthritis in patients with psoriasis: A systematic review and meta-analysis of observational and clinical studies. J Am Acad Dermatol. 2019;80:251-265.e19. - PubMed
-
- Prey S, Paul C, Bronsard V, et al. Assessment of risk of psoriatic arthritis in patients with plaque psoriasis: A systematic review of the literature. J Eur Acad Dermatol Venereol. 2010;24(Suppl 2):31-35. - PubMed
-
- Rahmati S, Li Q, Rahman P, Chandran V. Insights into the pathogenesis of psoriatic arthritis from genetic studies. Semin Immunopathol. 2021;43:221-234. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous