

Operative and nonoperative outcomes in patients with trisomy 13 and 18 with congenital heart disease
- PMID: 39296445
- PMCID: PMC11405994
- DOI: 10.1016/j.xjon.2024.06.007
Operative and nonoperative outcomes in patients with trisomy 13 and 18 with congenital heart disease
Abstract
Objective: To evaluate the short- and long-term outcomes of cardiac repair versus nonoperative management in patients with trisomy 13 and trisomy 18 with congenital heart disease.
Methods: An institutional review board-approved, retrospective review was undertaken to identify all patients admitted with trisomy 13/18 and congenital heart disease. Patients were divided into 2 cohorts (operated vs nonoperated) and compared.
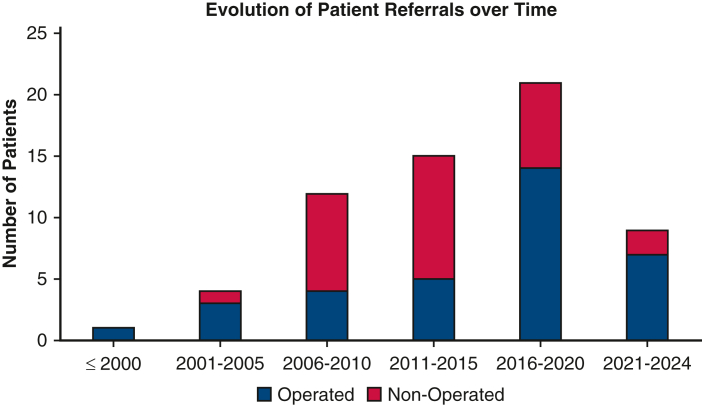
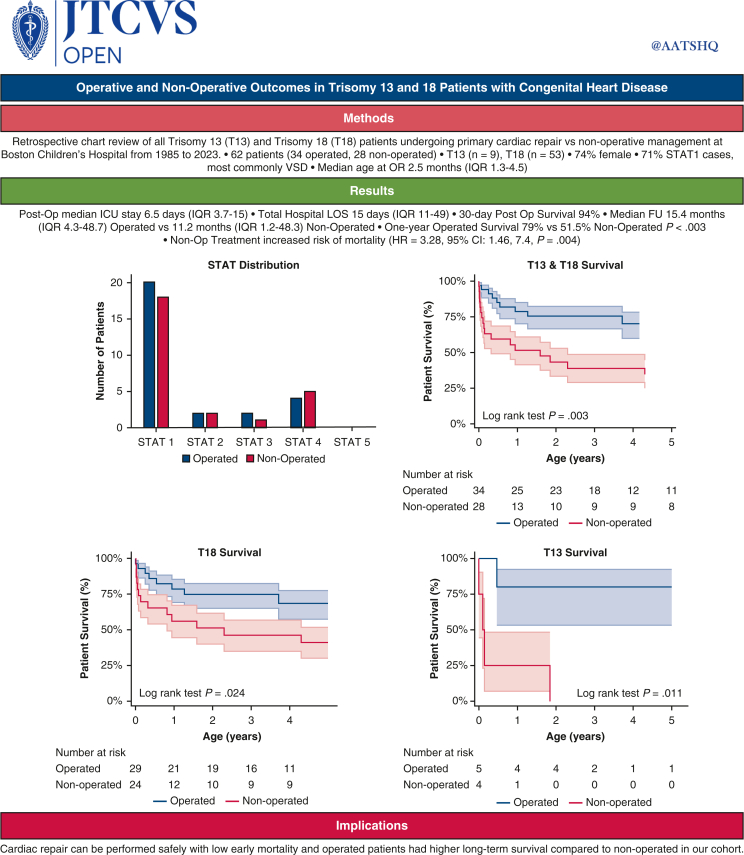
Results: Between 1985 and 2023, 62 patients (34 operated and 28 nonoperated) with trisomy 13 (n = 9) and trisomy 18 (n = 53) were identified. The operated cohort was 74% girls, underwent mainly The Society of Thoracic Surgeons-European Association for Cardio-Thoracic Surgery mortality category 1 procedures (n = 24 [71%]) at a median age of 2.5 months (interquartile range [IQR], 1.3-4.5 months). This compares with the nonoperative cohort where 64% (n = 18) would have undergone The Society of Thoracic Surgeons-European Association for Cardio-Thoracic Surgery mortality category 1 procedures if surgery would have been elected. The most common diagnosis was ventricular septal defect. Postoperative median intensive care unit stay was 6.5 days (IQR, 3.7-15 days) with a total hospital length of stay of 15 days (IQR, 11-49 days). Thirty-day postoperative survival was 94%. There were 5 in-hospital deaths in the operated and 7 in the nonoperated cohort. Median follow-up was 15.4 months (IQR, 4.3-48.7 months) for the operated and 11.2 months (IQR, 1.2-48.3 months) for the nonoperated cohorts. One-year survival was 79% operated versus 51.5% nonoperated (P < .003). Nonoperative treatment had an increased risk of mortality (hazard ratio, 3.28; 95% CI, 1.46-7.4; P = .004).
Conclusions: Controversy exists regarding the role of primary cardiac repair in patients with trisomy 13/18 and congenital heart disease. Cardiac repair can be performed safely with low early mortality and operated patients had higher long-term survival compared with nonoperated in our cohort.
Keywords: congenital heart disease; trisomy 13; trisomy 18.
© 2024 The Author(s).
Conflict of interest statement
John David Korngiebel Trust Fund as a source of funding for this article. The authors reported no conflicts of interest. The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
Figures





References
-
- Irving C., Richmond S., Wren C., Longster C., Embleton N.D. Changes in fetal prevalence and outcome for trisomies 13 and 18: a population-based study over 23 years. J Matern Fetal Neonatal Med. 2011;24(1):137–141. - PubMed
-
- Pont S.J., Robbins J.M., Bird T.M., et al. Congenital malformations among liveborn infants with trisomies 18 and 13. Am J Med Genet A. 2006;140(16):1749–1756. - PubMed
-
- Carey J.C. In: Management of Genetic Syndromes. Cassidy S.B., Allanson J.E., editors. John Wiley & Sons; 2010. Trisomy 18 and trisomy 13 syndromes; pp. 807–823.
-
- Matsuoka R., Misugi K., Goto A., et al. Congenital heart anomalies in the trisomy 18 syndrome with reference to congenital polyvalvular disease. Am J Med Genet. 1983;14(4):657–658. - PubMed
LinkOut - more resources
Full Text Sources
