

Acute brain injury risk prediction models in venoarterial extracorporeal membrane oxygenation patients with tree-based machine learning: An Extracorporeal Life Support Organization Registry analysis
- PMID: 39296456
- PMCID: PMC11405982
- DOI: 10.1016/j.xjon.2024.06.001
Acute brain injury risk prediction models in venoarterial extracorporeal membrane oxygenation patients with tree-based machine learning: An Extracorporeal Life Support Organization Registry analysis
Abstract
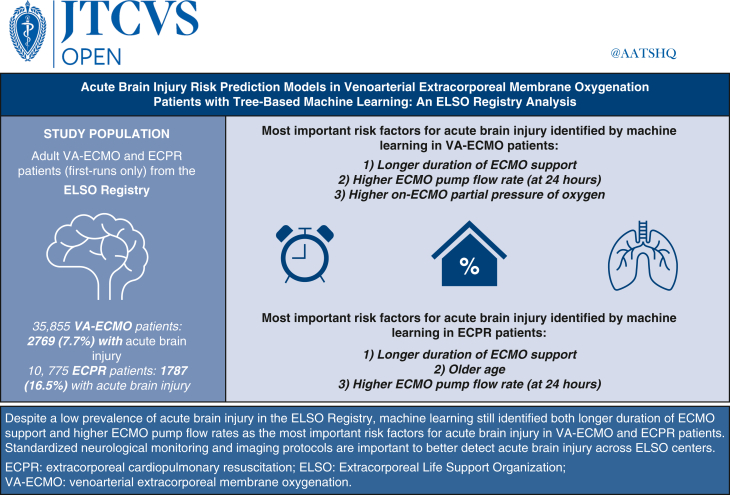
Objective: We aimed to determine if machine learning can predict acute brain injury and to identify modifiable risk factors for acute brain injury in patients receiving venoarterial extracorporeal membrane oxygenation.
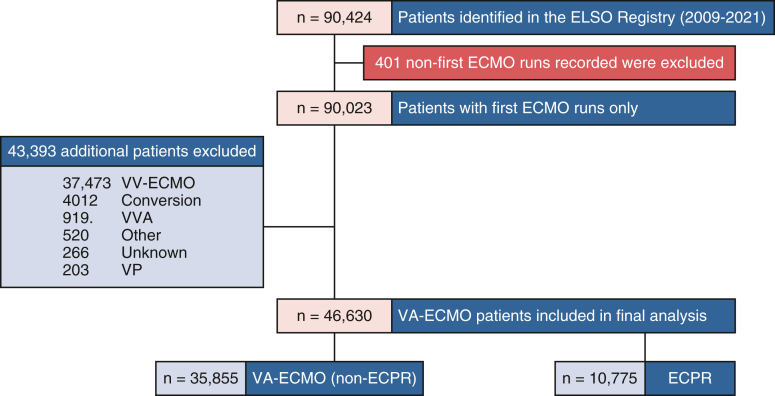
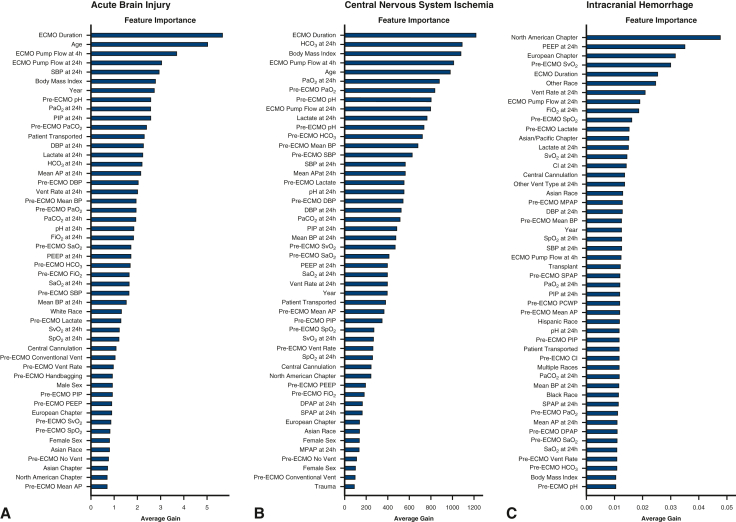
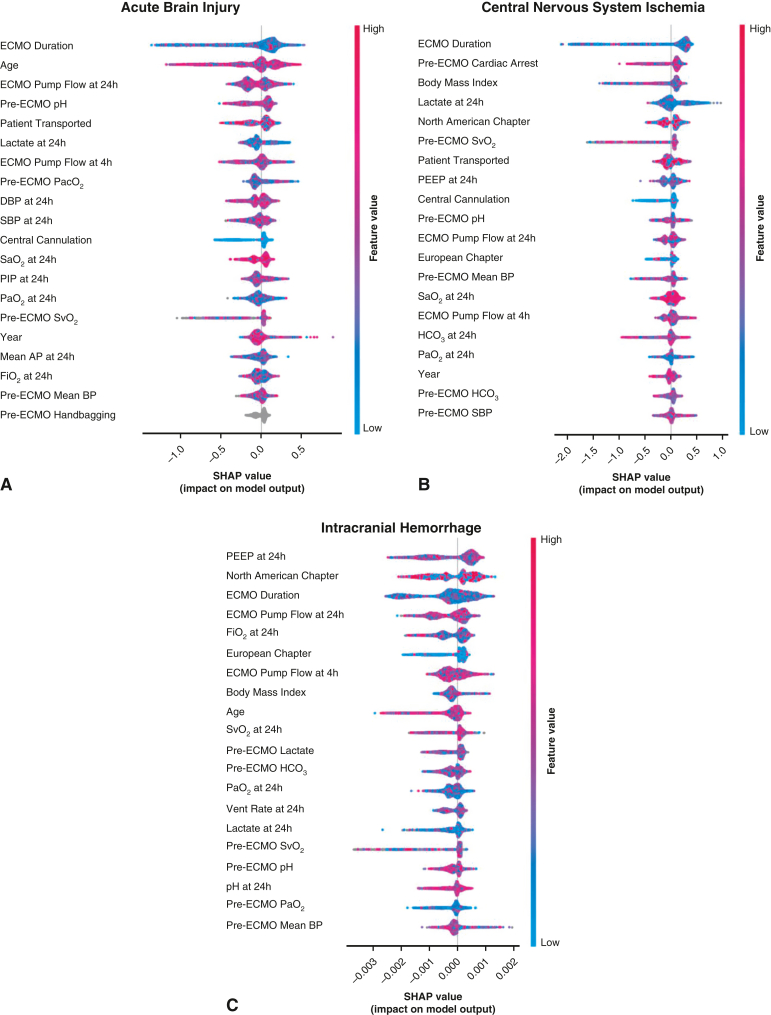
Methods: We included adults (age ≥18 years) receiving venoarterial extracorporeal membrane oxygenation or extracorporeal cardiopulmonary resuscitation in the Extracorporeal Life Support Organization Registry (2009-2021). Our primary outcome was acute brain injury: central nervous system ischemia, intracranial hemorrhage, brain death, and seizures. We used Random Forest, CatBoost, LightGBM, and XGBoost machine learning algorithms (10-fold leave-1-out cross-validation) to predict and identify features most important for acute brain injury. We extracted 65 total features: demographics, pre-extracorporeal membrane oxygenation/on-extracorporeal membrane oxygenation laboratory values, and pre-extracorporeal membrane oxygenation/on-extracorporeal membrane oxygenation settings.
Results: Of 35,855 patients receiving venoarterial extracorporeal membrane oxygenation (nonextracorporeal cardiopulmonary resuscitation) (median age of 57.8 years, 66% were male), 7.7% (n = 2769) experienced acute brain injury. In venoarterial extracorporeal membrane oxygenation (nonextracorporeal cardiopulmonary resuscitation), the area under the receiver operator characteristic curves to predict acute brain injury, central nervous system ischemia, and intracranial hemorrhage were 0.67, 0.67, and 0.62, respectively. The true-positive, true-negative, false-positive, false-negative, positive, and negative predictive values were 33%, 88%, 12%, 67%, 18%, and 94%, respectively, for acute brain injury. Longer extracorporeal membrane oxygenation duration, higher 24-hour extracorporeal membrane oxygenation pump flow, and higher on-extracorporeal membrane oxygenation partial pressure of oxygen were associated with acute brain injury. Of 10,775 patients receiving extracorporeal cardiopulmonary resuscitation (median age of 57.1 years, 68% were male), 16.5% (n = 1787) experienced acute brain injury. The area under the receiver operator characteristic curves for acute brain injury, central nervous system ischemia, and intracranial hemorrhage were 0.72, 0.73, and 0.69, respectively. Longer extracorporeal membrane oxygenation duration, older age, and higher 24-hour extracorporeal membrane oxygenation pump flow were associated with acute brain injury.
Conclusions: In the largest study predicting neurological complications with machine learning in extracorporeal membrane oxygenation, longer extracorporeal membrane oxygenation duration and higher 24-hour pump flow were associated with acute brain injury in nonextracorporeal cardiopulmonary resuscitation and extracorporeal cardiopulmonary resuscitation venoarterial extracorporeal membrane oxygenation.
Keywords: Extracorporeal Life Support Organization; acute brain injury; extracorporeal membrane oxygenation; machine learning; neurological complications.
© 2024 The Author(s).
Conflict of interest statement
D.B. receives research support from and consults for LivaNova; has been on the medical advisory boards for Xenios, Medtronic, Inspira, and Cellenkos; is the President-elect of the ELSO and the Chair of the Executive Committee of the International ECMO Network (ECMONet); and writes for UpToDate. C.E.V. has been a consultant or served on advisory boards for Merck, Janssen, and Regeneron, outside of the submitted work. S.M.C. is supported by the National Heart, Lung, and Blood Institute (1K23HL157610) and Hyperfine (SAFE MRI ECMO study). All other authors reported no conflicts of interest. The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
Figures







Update of
-
Predicting Acute Brain Injury in Venoarterial Extracorporeal Membrane Oxygenation Patients with Tree-Based Machine Learning: Analysis of the Extracorporeal Life Support Organization Registry.Res Sq [Preprint]. 2024 Jan 11:rs.3.rs-3848514. doi: 10.21203/rs.3.rs-3848514/v1. Res Sq. 2024. Update in: JTCVS Open. 2024 Jun 08;20:64-88. doi: 10.1016/j.xjon.2024.06.001. PMID: 38260374 Free PMC article. Updated. Preprint.
References
-
- Thiagarajan R.R., Barbaro R.P., Rycus P.T., et al. Extracorporeal life support organization registry international report 2016. ASAIO J. 2017;63(1):60–67. - PubMed
-
- Cho S.M., Canner J., Chiarini G., et al. Modifiable risk factors and mortality from ischemic and hemorrhagic strokes in patients receiving venoarterial extracorporeal membrane oxygenation: results from the extracorporeal life support organization registry. Crit Care Med. 2020;48(10):e897–e905. - PMC - PubMed
-
- Ong C.S., Etchill E., Dong J., et al. Neuromonitoring detects brain injury in patients receiving extracorporeal membrane oxygenation support. J Thorac Cardiovasc Surg. 2023;165:2104–2110.e1. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
