

Clinical decision support systems for maternity care: a systematic review and meta-analysis
- PMID: 39296586
- PMCID: PMC11408819
- DOI: 10.1016/j.eclinm.2024.102822
Clinical decision support systems for maternity care: a systematic review and meta-analysis
Abstract
Background: The use of Clinical Decision Support Systems (CDSS) is increasing throughout healthcare and may be able to improve safety and outcomes in maternity care, but maternity care has key differences to other disciplines that complicate the use of CDSS. We aimed to identify evaluated CDSS and synthesise evidence of their impact on maternity care.
Methods: We conducted a systematic review for articles published before 24th May 2024 that described i) CDSS that ii) investigated the impact of their use iii) in maternity settings. Medline, CINAHL, CENTRAL and HMIC were searched for articles relating to evaluations of CDSS in maternity settings, with forward- and backward-citation tracing conducted for included articles. Risk of bias was assessed using the Mixed Methods Assessment Tool, and CDSS were described according to the clinical problem, purpose, design, and technical environment. Quantitative results from articles reporting appropriate data were meta-analysed to estimate odds of a CDSS achieving its desired outcome using a multi-level random effects model, first by individual CDSS and then across all CDSS. PROSPERO ID: CRD42022348157.
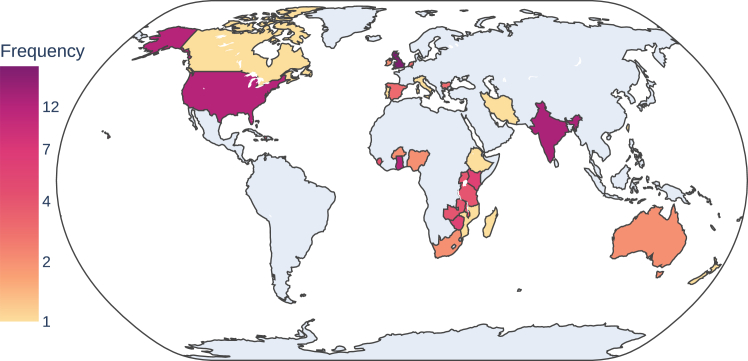
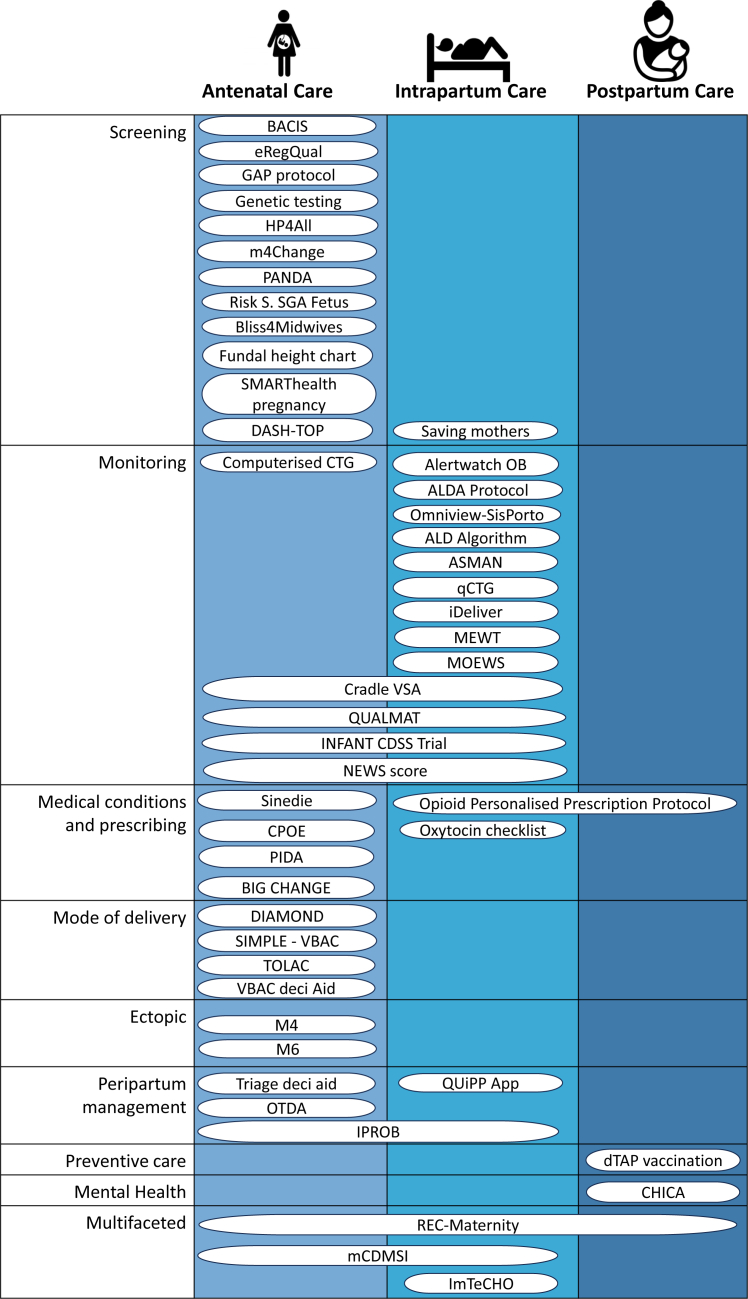
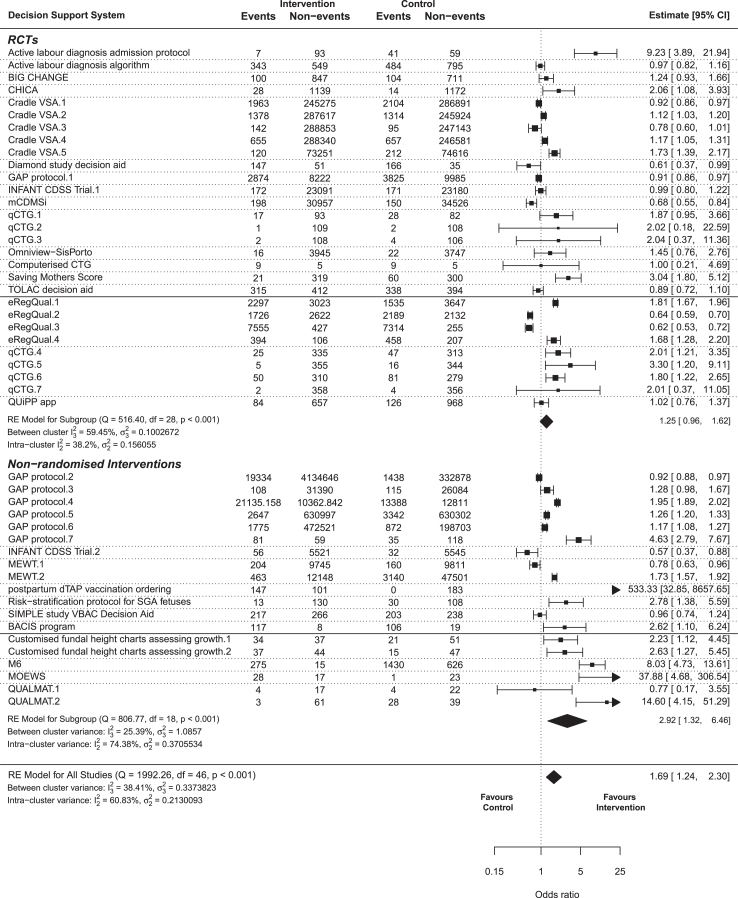
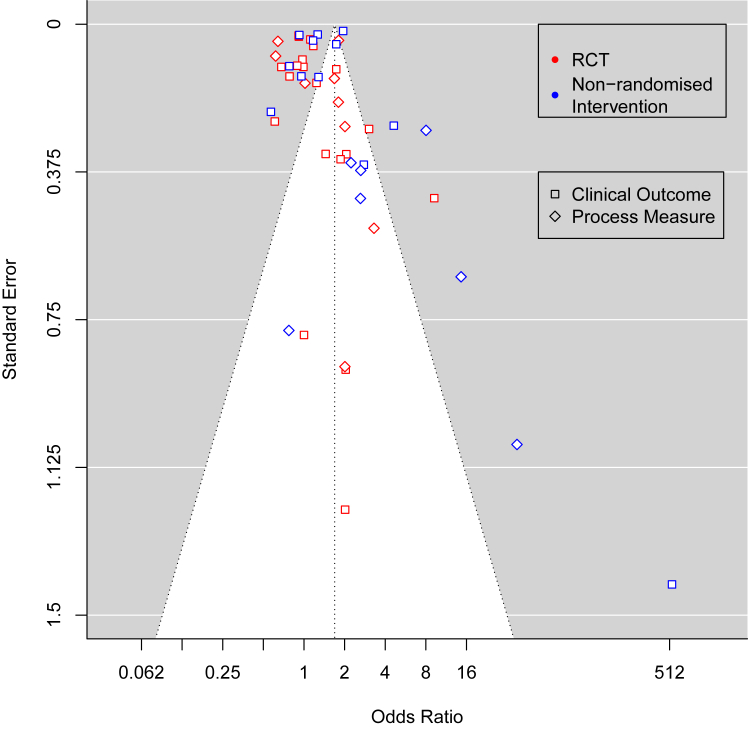
Findings: We screened 12,039 papers and included 87 articles describing 47 unique CDSS. 24 articles (28%) described randomised controlled trials, 30 (34%) described non-randomised interventional studies, 10 (11%) described mixed methods studies, 10 (11%) described qualitative studies, 7 (8%) described quantitative descriptive studies, and 7 (8%) described economic evaluations. 49 (56%) were in High-Income Countries and 38 (44%) in Low- and Middle-Income countries, with no CDSS trialled in both income categories. Meta-analysis of 35 included studies found an odds ratio for improved outcomes of 1.69 (95% confidence interval 1.24-2.30). There was substantial variation in effects, aims, CDSS types, context, study designs, and outcomes.
Interpretation: Most CDSS evaluations showed improvements in outcomes, but there was heterogeneity in all aspects of design and evaluation of systems. CDSS are increasingly important in delivering healthcare, and Electronic Health Records and mHealth will increase their availability, but traditional epidemiological methods may be limited in guiding design and demonstrating effectiveness due to rapid CDSS development lifecycles and the complex systems in which they are embedded. Development methods that are attentive to context, such as Human Centred Design, will help to meet this need.
Funding: None.
Keywords: Clinical decision support; Maternity; Obstetrics; Systematic review; mHealth.
© 2024 The Author(s).
Conflict of interest statement
WPS is a council member Royal College of Obstetricians and Gynecologists. MS and KN are directors of OpenClinical CIC, a not-for-profit organisation that seeks to promote the use of Clinical Decision Support technologies. MS owns stock and received royalties from Deontics Ltd., a Clinical Decision Support company whose products are not included in the reviewed papers. JSC received grant and contract funding from National Institute for Health and Care Research, Youth Endowment Fund, College of Policing, University of Birmingham, Birmingham City Council, Home Office (UK). BT received grant and contract funding from NIHR and UKRI/MRC. KN received grant and contract funding from NIHR, UKRI/MRC, Kennedy Trust for Rheumatology Research, Health Data Research UK, Wellcome Trust, European Regional Development Fund, Institute for Global Innovation, Boehringer Ingelheim, Action Against Macular Degeneration Charity, Midlands Neuroscience Teaching and Development Funds, South Asian Health Foundation, Vifor Pharma, College of Police, and CSL Behring, and consulting fees from BI, Sanofi, CEGEDIM and MSD.
Figures

References
-
- The United Nations . 2015. The Millenium development goals report. United Nations, New York.
-
- United Nations The 17 goals | sustainable development. https://sdgs.un.org/goals
-
- Trends in maternal mortality 2000 to 2020: estimates by WHO, UNICEF, UNFPA. World Bank Group and UNDESA/Population Division; 2023. https://iris.who.int/bitstream/handle/10665/366225/9789240068759-eng.pdf...
-
- Khalil A, Samara A, O’Brien P, Coutinho CM, Quintana SM, Ladhani SN. A call to action: the global failure to effectively tackle maternal mortality rates. Lancet Global Health. 2023;11:e1165–e1167. - PubMed
-
- Shaw D, Guise JM, Shah N, et al. Drivers of maternity care in high-income countries: can health systems support woman-centred care? Lancet. 2016;388:2282–2295. - PubMed
LinkOut - more resources
Full Text Sources
