

Refractory massive chylothorax following robot-assisted laparoscopic splenectomy with pericardial devascularization treated with trans-jugular intrahepatic portosystemic shunt: a case report
- PMID: 39296890
- PMCID: PMC11408172
- DOI: 10.3389/fmed.2024.1420157
Refractory massive chylothorax following robot-assisted laparoscopic splenectomy with pericardial devascularization treated with trans-jugular intrahepatic portosystemic shunt: a case report
Abstract
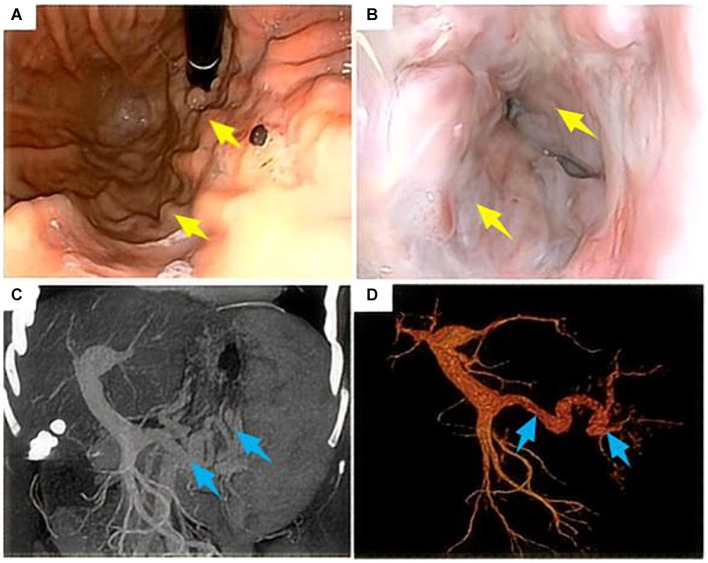
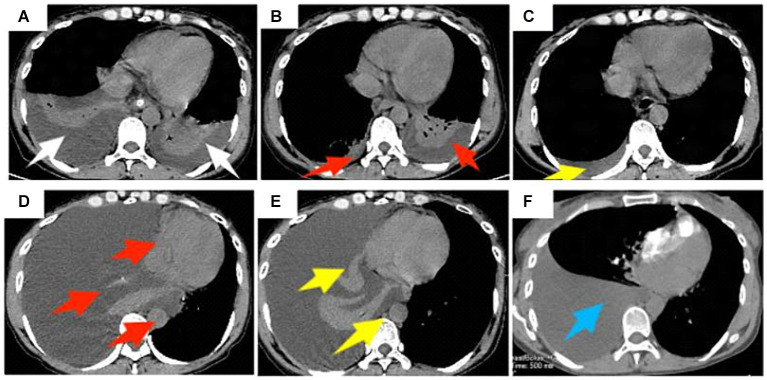
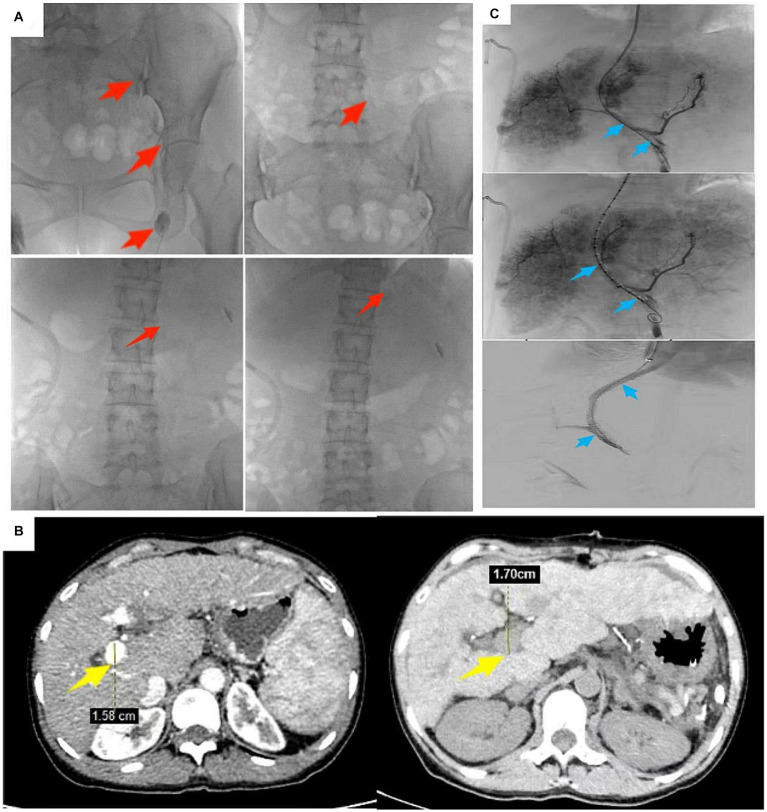
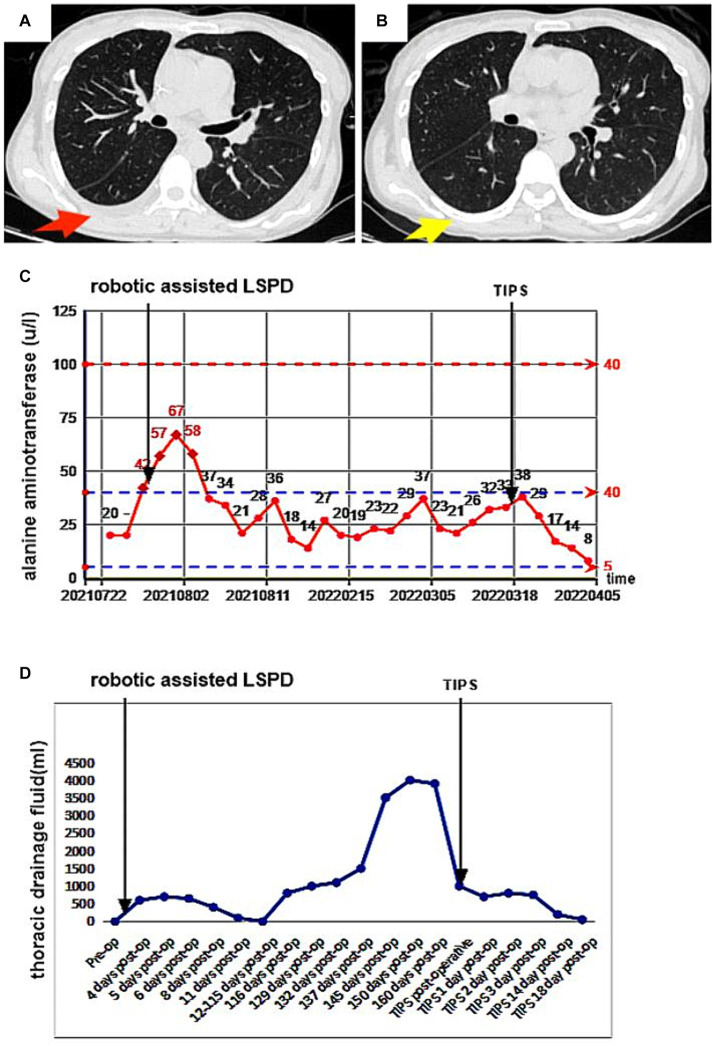
The development of a chylothorax after robot-assisted laparoscopic splenectomy combined with pericardial devascularization (LSPD) is rare. The robot-assisted procedure is similar to the standard LSPD, but surgeons must remain vigilant about potential chylothorax caused by recurrence of portal hypertension in patients with cirrhosis, an event that leads to variceal bleeding in the gastric fundus or a massive chylothorax caused by a thoracic duct fistula. We report a rare case of massive chylothorax after robot-assisted LSPD and review the literature to help elucidate the mechanisms of portal hypertension after LSPD, reduce surgical complications, and improve long-term patient outcomes. After LSPD, portal pressure monitoring, coagulation function testing, and portal vein CT imaging help in excluding portal vein thromboses and ensuring appropriate anticoagulation to reduce the development of thoracic duct fistulas. If portal hypertension recurs after surgery and a high-output chylothorax develops, conservative treatment becomes ineffective. Treatment with an active trans-jugular intrahepatic portosystemic shunt (TIPS) is recommended to lower the portal pressure.
Keywords: LSPD; gastric fundus varices; massive chylothorax; portal hypertension; tips.
Copyright © 2024 Deng and Xia.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Bao H, He Q, Dai N, Ye R, Zhang Q. Retrospective study to compare selective decongestive devascularization and gastrosplenic shunt versus splenectomy with pericardial devascularization for the treatment of patients with esophagogastric varices due to cirrhotic portal hypertension. Med Sci Monit. (2017) 23:2788–95. doi: 10.12659/msm.904660, PMID: - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources