

Mixed thyrotropin-secreting pituitary neuroendocrine tumor coexisting with Graves' disease: a case report
- PMID: 39296905
- PMCID: PMC11408738
- DOI: 10.3389/fmed.2024.1436400
Mixed thyrotropin-secreting pituitary neuroendocrine tumor coexisting with Graves' disease: a case report
Abstract
Background: Thyrotropin (TSH)-secreting pituitary neuroendocrine tumors (PitNETs) are recognized as a rare disease. Mixed TSH PitNETs account for 20-25% of TSH PitNETs. This study aimed to report an extremely rare case of a mixed TSH PitNET coexisting with Graves' disease (GD) and also to review the literature.
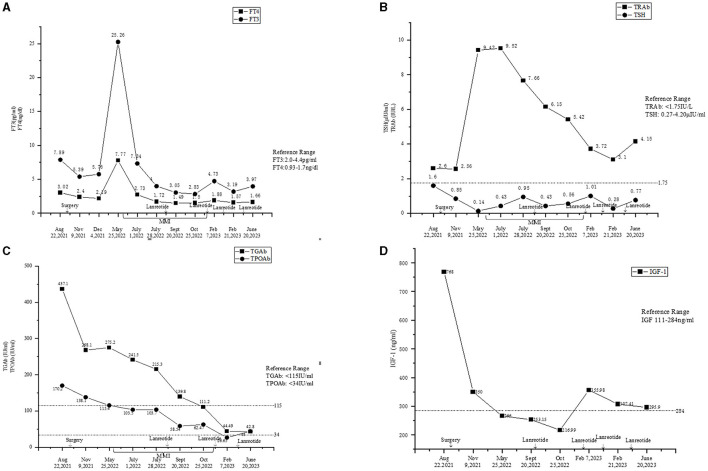
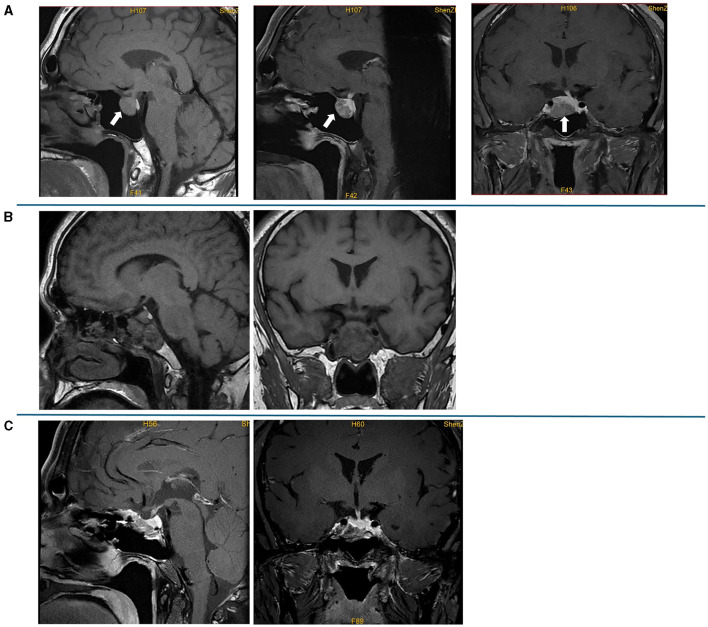
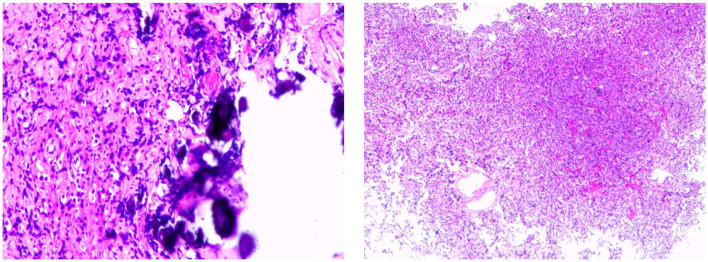
Case presentation: A 36-year-old male patient presented with elevated levels of free triiodothyronine (FT3), free thyroxine (FT4), and insulin-like growth factor 1 (IGF-1) but a non-suppressed thyroid-stimulating hormone (TSH) level. His anti-thyroglobulin antibody (TgAb), anti-thyroid peroxidase autoantibody (TPOAb), and thyrotropin receptor antibody (TRAb) tests were positive. Symptoms of palpitations, hyperhidrosis, heat intolerance, and irritability appeared 2 years before his admission. However, he showed neither any signs nor any symptoms of acromegaly. The contrast-enhanced pituitary magnetic resonance imaging (MRI) showed enlargement of the pituitary fossa, with an irregular abnormal signal mass. The patient underwent endoscopic pituitary tumor resection via a transsphenoidal approach. The postoperative pathology suggested a mixed pituitary adenoma. At 8 months after the surgery, the patient had a postoperative recurrence of hyperthyroidism, and methimazole (MMI) was then administered. The recurrence of the TSH PitNET was confirmed by the positron emission tomography-computed tomography (PET-CT), which was performed 11 months after the surgery, and treatment with lanreotide was initiated. Gradually, his levels of FT3, FT4, TSH, TPOAb, and TgAb became normal and the levels of TRAb and IGF-1 improved.
Conclusion: When the circulating levels of both FT4 and FT3 were upregulated, non-suppressed TSH levels and positive thyroid antibodies were found. TSH PitNETs coexisting with GD should be carefully taken into account to avoid the potential risk of treatment-induced tumor progression.
Keywords: Graves' disease; autoimmune thyroid disease; mixed pituitary neuroendocrine tumor; thyroid antibodies; thyrotropin-secreting pituitary neuroendocrine tumor.
Copyright © 2024 Huang, Wen, Liang and Xu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Kamoi K, Mitsuma T, Sato H, Yokoyama M, Washiyama K, Tanaka R, et al. Hyperthyroidism caused by a pituitary thyrotrophin-secreting tumour with excessive secretion of thyrotrophin-releasing hormone and subsequently followed by Graves' disease in a middle-aged woman. Acta Endocrinol (Copenh). (1985) 110:373–82. 10.1530/acta.0.1100373 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous