

A phase III study to access the safety and efficacy of prolgolimab 250 mg fixed dose administered every 3 weeks versus prolgolimab 1 mg/kg every 2 weeks in patients with metastatic melanoma (FLAT)
- PMID: 39296979
- PMCID: PMC11408354
- DOI: 10.3389/fonc.2024.1385685
A phase III study to access the safety and efficacy of prolgolimab 250 mg fixed dose administered every 3 weeks versus prolgolimab 1 mg/kg every 2 weeks in patients with metastatic melanoma (FLAT)
Abstract
Background: Prolgolimab is the first Russian PD-1 inhibitor approved for the first-line treatment of unresectable or metastatic melanoma and advanced non-small cell lung cancer. It was approved in two weight-based regimens of 1 mg/kg Q2W and 3 mg/kg Q3W, but because of re-evaluation of weight-based dosing paradigm, studying of a fixed-dose regimen was considered perspective.
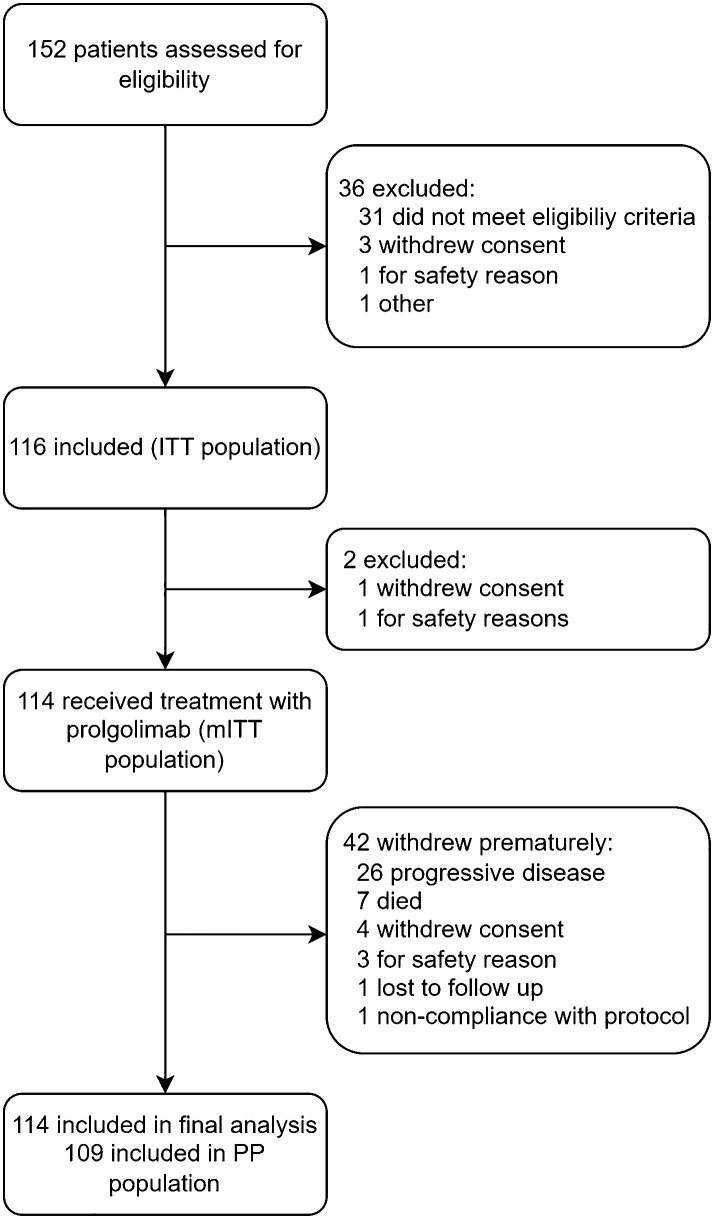
Methods: We conducted a multicenter, single-arm, open-label efficacy, pharmacokinetics, and safety study to obtain data that would allow the approval of the new flat dosing regimen of prolgolimab in patients with previously untreated unresectable or metastatic melanoma (BCD-100-8/FLAT, NCT05783882). The primary objective was to prove the non-inferiority of prolgolimab 250 mg Q3W versus prolgolimab 1 mg/kg Q2W for the treatment of patients with unresectable or metastatic melanoma in terms of ORR according to RECIST 1.1. Patients from the MIRACULUM study (BCD-100-2/MIRACULUM, NCT03269565) comprised a historical control group.
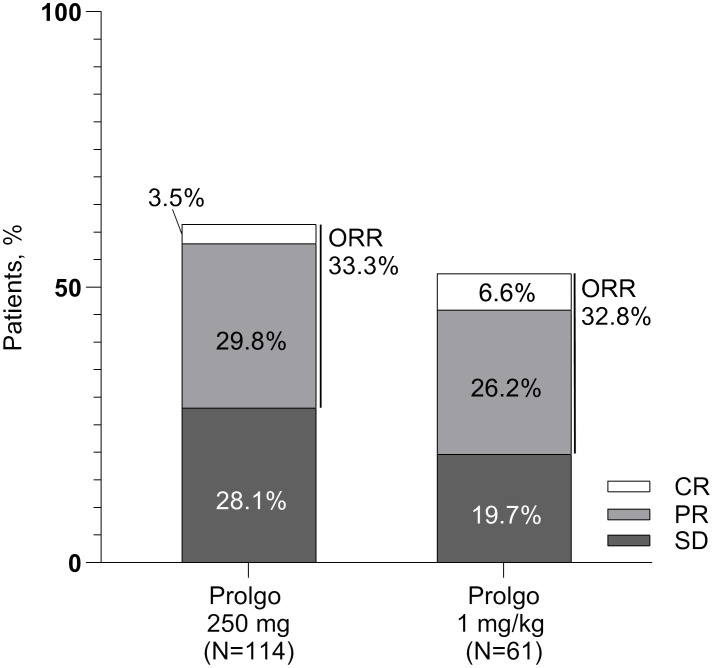
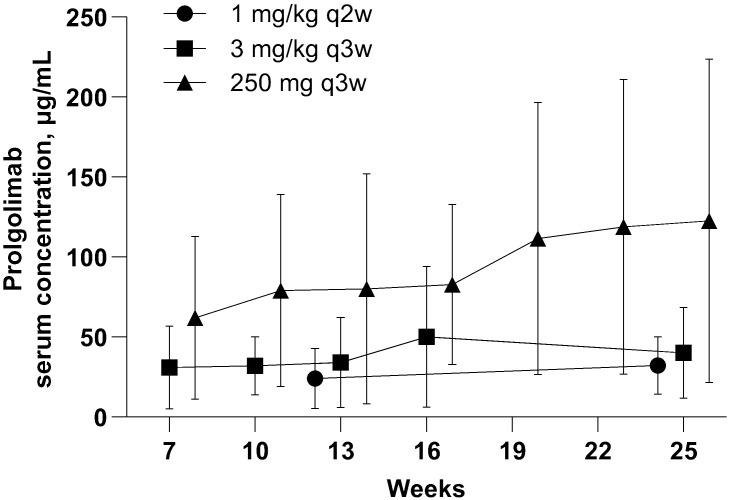
Results: One hundred fourteen patients received prolgolimab 250 mg Q3W, and 61 patients received prolgolimab (Prolgo) 1 mg/kg Q2W (historical control). Objective response was achieved by 33.3% [95% confidence interval (CI): 24.8, 42.8] of patients in the Prolgo 250 mg group compared with 32.8% (95% CI: 21.3, 46.0) of patients in the Prolgo 1 mg/kg group. Risk difference was 0.00, 95% CI (-0.12; NA), p = 0.0082. Both regimens were well tolerated, and safety profiles were comparable. The pharmacokinetic analysis (PK) showed that the regimen with the fixed dose of 250 mg Q3W was characterized by higher PK parameters. The immunogenicity study did not detect binding antibodies to prolgolimab in any of the subjects.
Conclusion: The obtained results showed that the selected fixed dosing regimen of prolgolimab 250 mg Q3W is characterized by efficacy and safety parameters comparable to that observed for the 1 mg/kg Q2W regimen.
Keywords: PD-1 inhibitor; fixed dose; immunotherapy; melanoma; prolgolimab.
Copyright © 2024 Demidov, Kharkevich, Petenko, Moiseenko, Protsenko, Semiglazova, Zimina, Kovalenko, Fadeeva, Kirtbaya, Belogortsev, Tantsyrev, Odintsova, Nesterova, Vorontsova, Makarycheva, Linkova, Zinkina-Orikhan, Siliutina, Sorokina, Liaptseva, Chistyakov and Lutsky.
Conflict of interest statement
GK, NP, VM, SP, TS, AZ, NK, NF, DK, IB, DT, SO, AN, KV, YM, and LD report clinical trial investigator’s fee BCD-100-8/FLAT and honoraria from BIOCAD for participation as a speaker at scientific and educational meetings. YL, AZ-O, IS, AS, DL, VC, and AL are BIOCAD employees. The study was initiated, funded, and sponsored by JSC Biocad. Design and conduct of the study was undertaken by the sponsor in collaboration with investigators. The study investigators and their respective research teams collected the data; JSC Biocad compiled the data for summation and analysis. All authors were responsible for data interpretation.
Figures
References
Associated data
LinkOut - more resources
Full Text Sources
Medical