

BMP10 reflects pre-capillary pulmonary hemodynamics: association of biomarkers and hemodynamic parameters in pulmonary hypertension
- PMID: 39297942
- PMCID: PMC11839876
- DOI: 10.1007/s00392-024-02546-8
BMP10 reflects pre-capillary pulmonary hemodynamics: association of biomarkers and hemodynamic parameters in pulmonary hypertension
Abstract
Background and aims: The role of biomarkers in diagnosing pulmonary hypertension (PH) and distinguishing between pre- and post-capillary PH remains poorly understood. We aimed to identify biomarkers with a strong association with mean pulmonary arterial pressure, mPAP (PH diagnosis) and pulmonary vascular resistance, PVR (pre-capillary component), but not with pulmonary arterial wedge pressure, PAWP (post-capillary component).
Methods: Blood samples were collected in patients undergoing right heart catheterization within a prospective cross-sectional study. Biomarkers measured included BMP10, NT-proBNP, ANG2, ESM1/endocan, FGF23, GDF15, IGFBP7, IL6, MyBPC3, proC3, and proC6/endotrophin. Primary outcomes were mPAP, PVR, and PAWP, while secondary outcomes included PH diagnosis (mPAP > 20 mmHg) and elevated PVR (> 2 Wood units). Multivariable linear and logistic regression models were used to assess the relationship between biomarkers and outcomes.
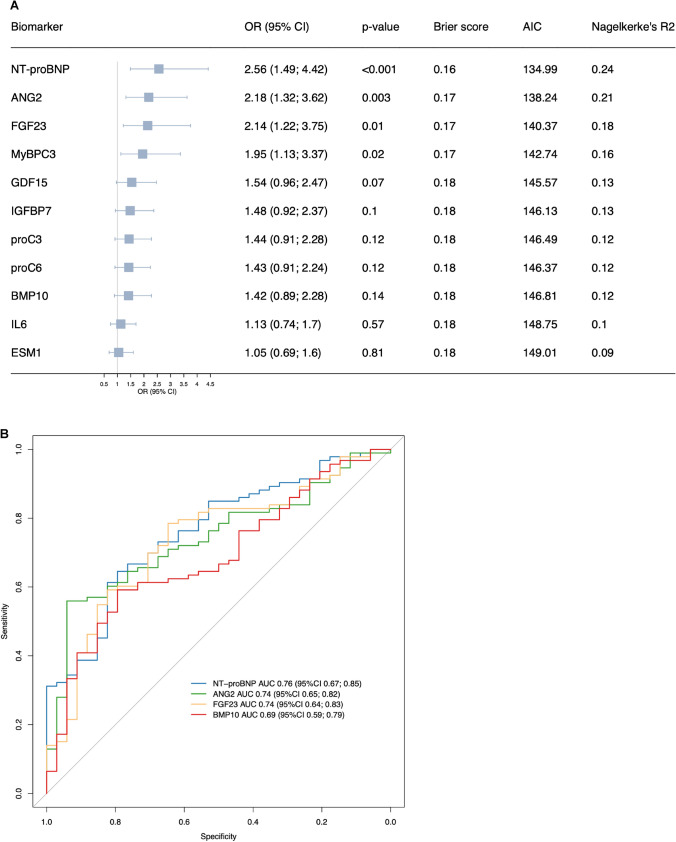
Results: Of the 127 patients included (age 66 ± 13 years, 54% female), 73% were diagnosed with PH. BMP10, NT-proBNP, ANG2, MyBPC3, and FGF23 showed a strong association with mPAP (p < 0.001). BMP10 and NT-proBNP were strongly associated with PVR (p < 0.001), while NT-proBNP and ANG2 were strongly associated with PAWP (p < 0.001). NT-proBNP had the strongest association with the diagnosis of PH (area under the curve = 0.76). BMP10 was the only biomarker associated with elevated PVR (OR 1.60, 95%CI 1.01-2.54, p = 0.04) but not with PAWP (p = 0.86).
Conclusions: Several biomarkers were strongly associated with mPAP, PAWP, and PVR. BMP10 was the only biomarker strongly associated with mPAP and PVR, but not with PAWP, thus reflecting the pre-capillary PH component. Measurement of BMP10 along with NT-proBNP may aid in diagnosing PH.
Keywords: BMP10; Biomarker; NT-proBNP; Pulmonary hypertension; Right heart catheterization.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: S. Aeschbacher received speaker fee from Roche Diagnostics outside of the submitted work. D. Conen received consultancy fees from Roche Diagnostics and Trimedics, as well as speaker fees from Servier. M. Kühne reports grants from the Swiss National Science Foundation (Grant numbers 33CS30_148474, 33CS30_177520, 32473B_176178, 32003B_197524), the Swiss Heart Foundation, the Foundation for Cardiovascular Research Basel and the University of Basel, grants from Bayer, grants from Pfizer, grants from Boston Scientific, grants from BMS, grants from Biotronik, grants and personal fees from Daiichi Sankyo. C. Müller received research support from the Swiss National Science Foundation, Swiss Heart Foundation, KTI, University Hospital Basel, University of Basel, Abbott, Astra Zeneca, Beckman Coulter, Brahms, Idorsia, Novartis, LSI Medience Corporation, Ortho Clinical Diagnostics, Quidel, Roche, Siemens, Singulex, SpinChip, and Sphingotec, all outside the current work and paid to the institution, as well as speaker honoraria/consulting honoraria from Abbott, Amgen, Astra Zeneca, Bayer, Boehringer Ingelheim, BMS, Idorsia, Novartis, Osler, Roche, Sanofi, SpinChip, and Singulex, all outside the current work and paid to the institution. S. Osswald received research grants from the Swiss National Science Foundation and Swiss Heart Foundation, Foundation for CardioVascular Research Basel, and F. Hoffmann-La Roche Ltd., and educational and speaker grants from F. Hoffmann-La Roche Ltd., Bayer, Novartis, Sanofi, AstraZeneca, Daiichi-Sankyo, and Pfizer. O. Pfister received speaker/consulting honoraria or travel support from Astra Zeneca, Bayer, Boehringer-Ingelheim, Daiichi Sankyo, Novartis, Pfizer, Sanofi, and Vifor Pharma. C.S. Zuern received travel support from Cardiomatics, Poland. The remaining authors have nothing to disclose.
Figures


References
-
- Humbert M, Kovacs G, Hoeper MM, Badagliacca R, Berger RMF, Brida M, Carlsen J, Coats AJS, Escribano-Subias P, Ferrari P, Ferreira DS, Ghofrani HA, Giannakoulas G, Kiely DG, Mayer E, Meszaros G, Nagavci B, Olsson KM, Pepke-Zaba J, Quint JK, Rådegran G, Simonneau G, Sitbon O, Tonia T, Toshner M, Vachiery JL, Vonk Noordegraaf A, Delcroix M, Rosenkranz S (2022) 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J 43:3618–3731 - PubMed
-
- Santema BT, Chan MMY, Tromp J, Dokter M, van der Wal HH, Emmens JE, Takens J, Samani NJ, Ng LL, Lang CC, van der Meer P, Ter MJM, Damman K, Dickstein K, Cleland JG, Zannad F, Anker SD, Metra M, van der Harst P, de Boer RA, van Veldhuisen DJ, Rienstra M, Lam CSP, Voors AA (2020) The influence of atrial fibrillation on the levels of NT-proBNP versus GDF-15 in patients with heart failure. Clin Res Cardiol 109:331–338 - PMC - PubMed
-
- Huber LC, Bye H, Brock M (2015) The pathogenesis of pulmonary hypertension—an update. Swiss Med Wkly 145:w14202 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
