

Preconception and Early-Pregnancy Body Mass Index in Women and Men, Time to Pregnancy, and Risk of Miscarriage
- PMID: 39298166
- PMCID: PMC11413718
- DOI: 10.1001/jamanetworkopen.2024.36157
Preconception and Early-Pregnancy Body Mass Index in Women and Men, Time to Pregnancy, and Risk of Miscarriage
Abstract
Importance: Obesity in women is associated with reduced fertility and an increased risk of miscarriage. These associations might also be present across the full range of body mass index (BMI) categories as well as among men.
Objective: To investigate the associations of preconception BMI in both partners with time to pregnancy and miscarriage.
Design, setting, and participants: This population-based prospective cohort study was conducted in Rotterdam, the Netherlands, between August 9, 2017, and July 1, 2021. A total of 3604 women and their partners were included from the preconception period onward with follow-up until birth. The date of analysis was July 12, 2024.
Exposure: Body mass index (calculated as weight in kilograms divided by height in meters squared) measured in preconception or early pregnancy.
Main outcome and measures: Fecundability, defined as the probability of conceiving within 1 month; subfertility, defined as time to pregnancy or duration of actively pursuing pregnancy of more than 12 months or use of assisted reproductive technology; and miscarriage, defined as pregnancy loss before 22 weeks of gestation. These measures were assessed using questionnaires and via the obstetric caregiver.
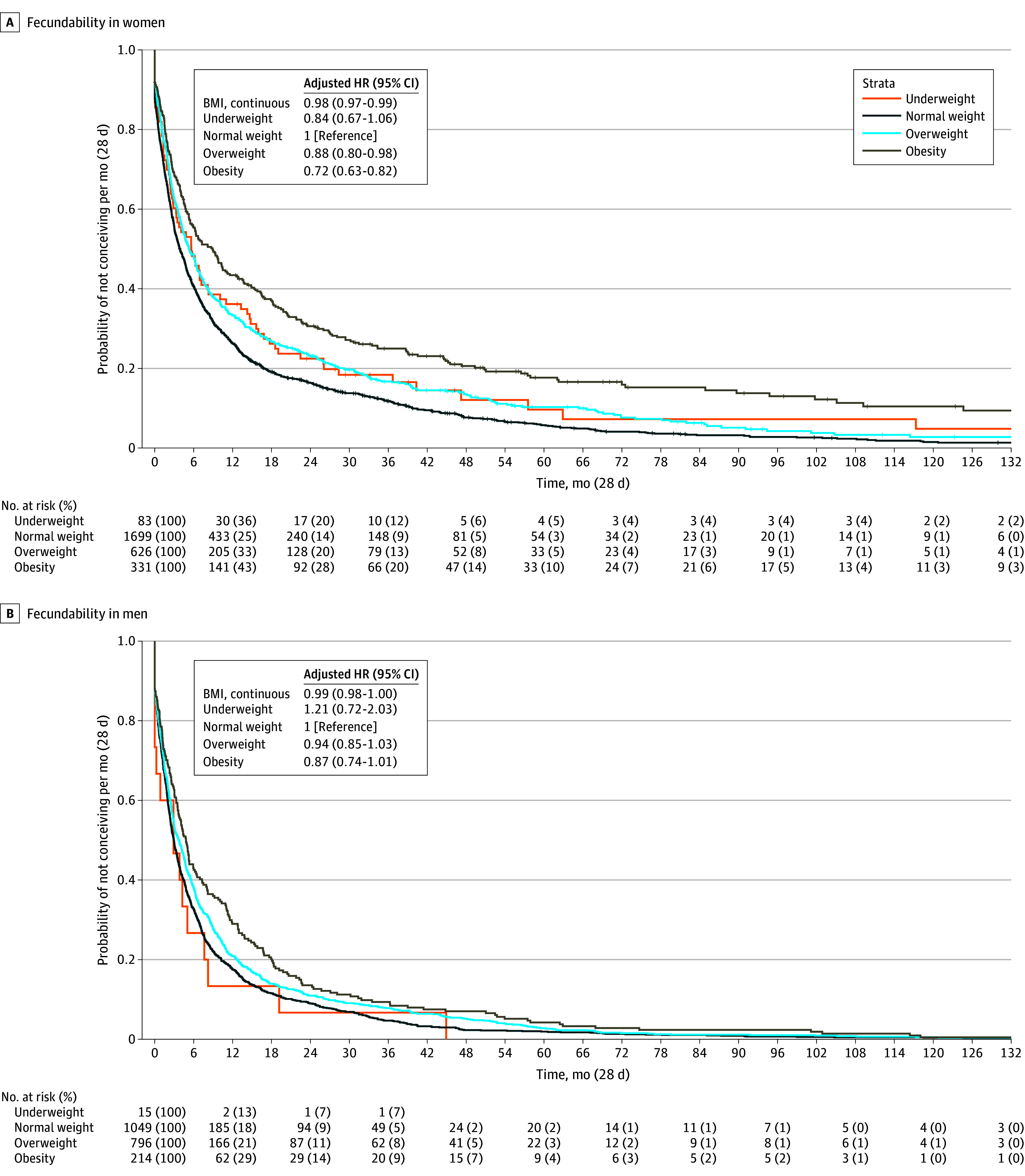
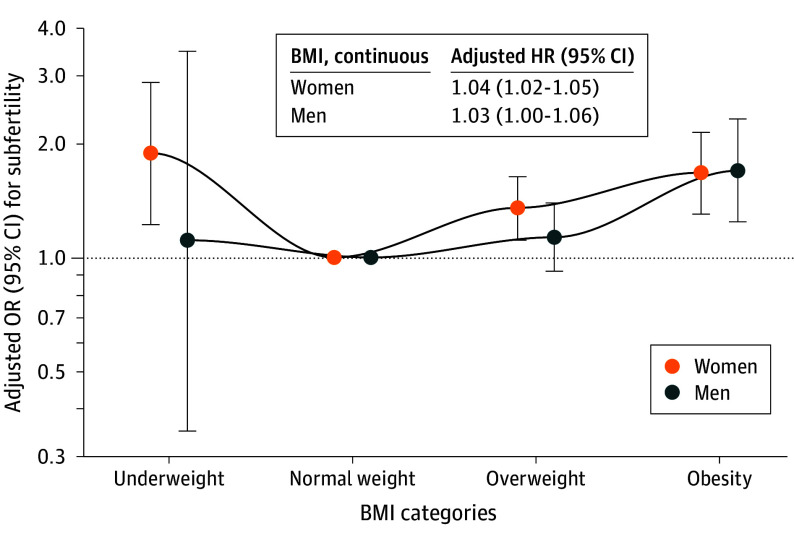
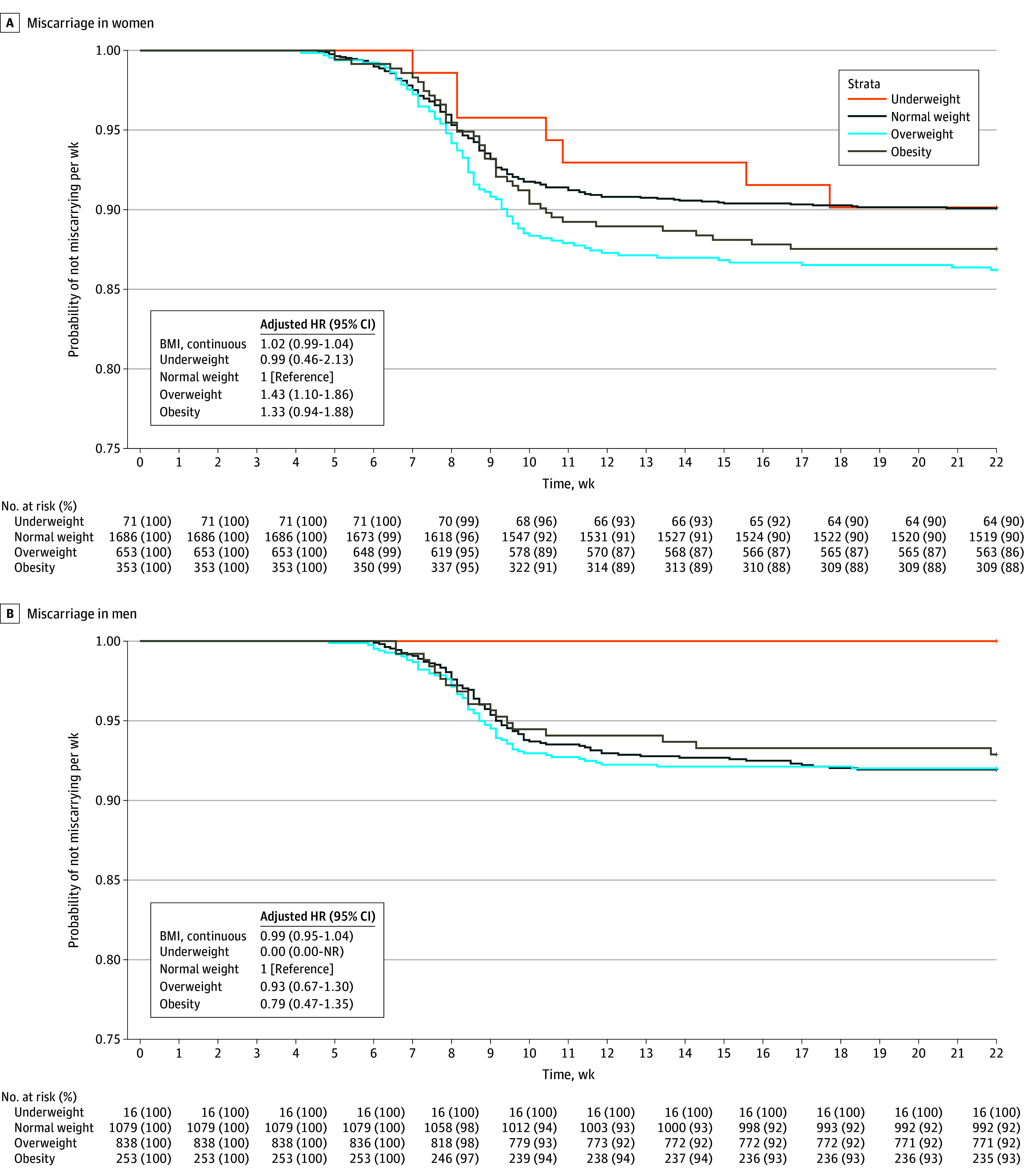
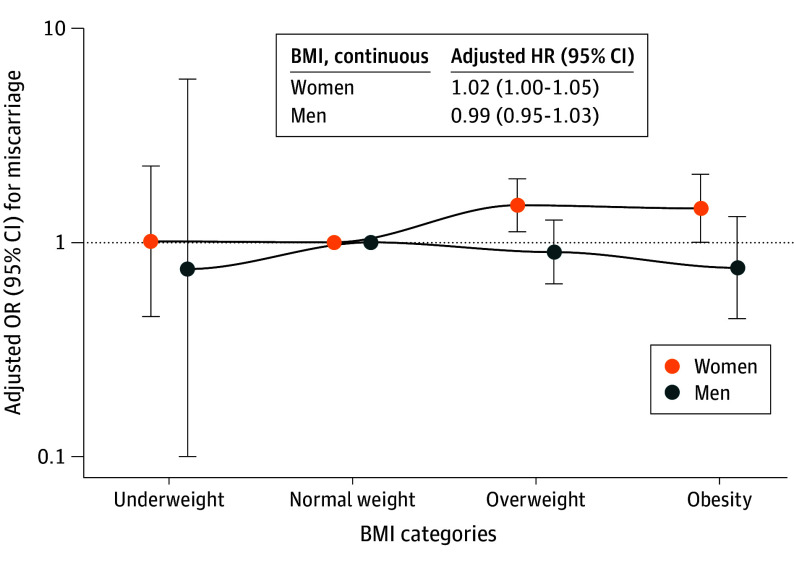
Results: The study population for time-to-pregnancy analyses consisted of 3033 episodes among women (median age, 31.6 years [IQR, 29.2-34.5 years]; median BMI, 23.5 [IQR, 21.2-26.5]) and 2288 episodes among men (median age, 33.4 years [IQR, 30.5-36.8 years]; median BMI, 24.9 [IQR, 23.0-27.4]). The study population for miscarriage analyses consisted of 2770 pregnancy episodes among women (median age, 31.5 years [IQR, 28.9-34.3 years]; median BMI, 23.5 [IQR, 21.3-26.7]) and 2189 pregnancy episodes among men (median age, 33.5 years [IQR, 30.4-36.8 years]; median BMI, 25.0 [IQR, 23.0-27.5]). Higher BMI in women and men was associated with lower fecundability: for every unit increase in BMI, fecundability decreased (fecundability ratio [FR]: women, 0.98 [95% CI, 0.97-0.99]; men, 0.99 [95% CI, 0.98-1.00]). Women with overweight (FR, 0.88 [95% CI, 0.80-0.98]) and obesity (FR, 0.72 [95% CI, 0.63-0.82]) had lower fecundability compared with women with normal weight. Compared with normal weight in women, underweight (odds ratio [OR], 1.88 [95% CI, 1.22-2.88]), overweight (OR, 1.35 [95% CI, 1.11-1.63]), and obesity (OR, 1.67 [95% CI, 1.30-2.13]) were associated with increased odds of subfertility. In men, obesity was associated with increased odds of subfertility (OR, 1.69 [95% CI, 1.24-2.31]). Compared with normal weight in women, overweight (OR, 1.49 [95% CI, 1.12-1.98]) and obesity (OR, 1.44 [95% CI, 1.00-2.08]) were associated with increased odds of miscarriage.
Conclusions and relevance: In this cohort study, BMI outside of the normal category in women and men during the preconception or early-pregnancy periods was associated with time to pregnancy and miscarriage. Optimizing BMI in women and men from the preconception period onward might be an important strategy to improve fertility outcomes.
Conflict of interest statement
Figures
References
-
- World Health Organization . WHO European Regional Obesity Report 2022. World Health Organization; 2022.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
