

Pivotal roles for cancer cell-intrinsic mPGES-1 and autocrine EP4 signaling in suppressing antitumor immunity
- PMID: 39298269
- PMCID: PMC11601572
- DOI: 10.1172/jci.insight.178644
Pivotal roles for cancer cell-intrinsic mPGES-1 and autocrine EP4 signaling in suppressing antitumor immunity
Abstract
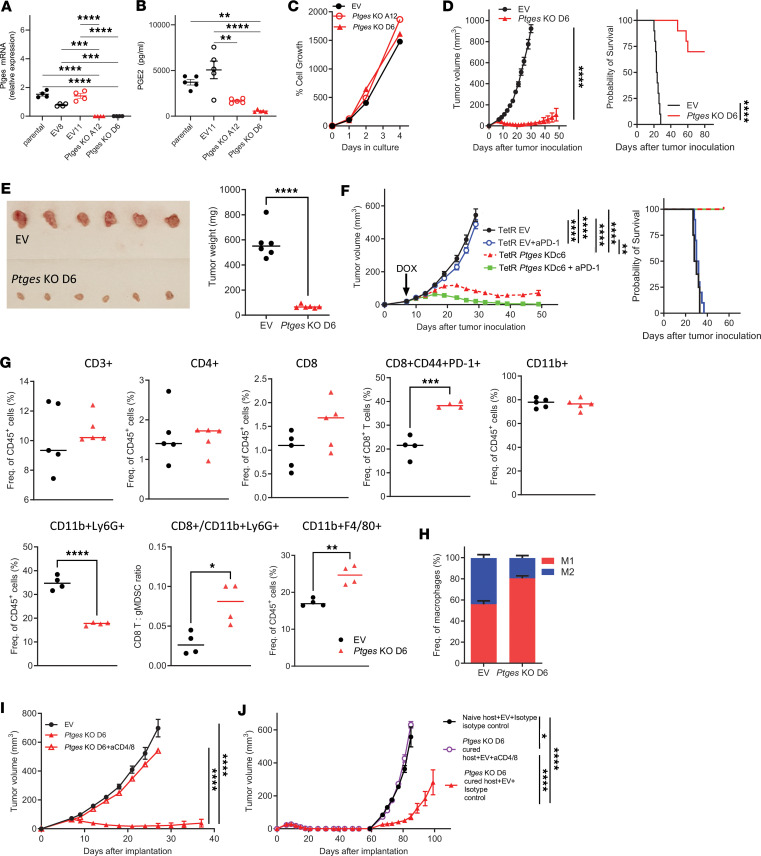
Tumor cell-derived prostaglandin E2 (PGE2) is a tumor cell-intrinsic factor that supports immunosuppression in the tumor microenvironment (TME) by acting on the immune cells, but the impact of PGE2 signaling in tumor cells on the immunosuppressive TME is unclear. We demonstrate that deleting the PGE2 synthesis enzyme or disrupting autocrine PGE2 signaling through EP4 receptors on tumor cells reverses the T cell-low, myeloid cell-rich TME, activates T cells, and suppresses tumor growth. Knockout (KO) of Ptges (the gene encoding the PGE2 synthesis enzyme mPGES-1) or the EP4 receptor gene (Ptger4) in KPCY (KrasG12D P53R172H Yfp CrePdx) pancreatic tumor cells abolished growth of implanted tumors in a T cell-dependent manner. Blockade of the EP4 receptor in combination with immunotherapy, but not immunotherapy alone, induced complete tumor regressions and immunological memory. Mechanistically, Ptges- and Ptger4-KO tumor cells exhibited altered T and myeloid cell attractant chemokines, became more susceptible to TNF-α-induced killing, and exhibited reduced adenosine synthesis. In hosts treated with an adenosine deaminase inhibitor, Ptger4-KO tumor cells accumulated adenosine and gave rise to tumors. These studies reveal an unexpected finding - a nonredundant role for the autocrine mPGES-1/PGE2/EP4 signaling axis in pancreatic cancer cells, further nominating mPGES-1 inhibition and EP4 blockade as immune-sensitizing therapy in cancer.
Keywords: Cancer immunotherapy; Eicosanoids; Immunology; Mouse models; Oncology.
Figures



References
-
- American Cancer Society. Cancer Facts & Figures 2023. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-... Accessed September 24, 2024.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
