

Immune profiling-based targeting of pathogenic T cells with ustekinumab in ANCA-associated glomerulonephritis
- PMID: 39300109
- PMCID: PMC11413367
- DOI: 10.1038/s41467-024-52525-w
Immune profiling-based targeting of pathogenic T cells with ustekinumab in ANCA-associated glomerulonephritis
Abstract
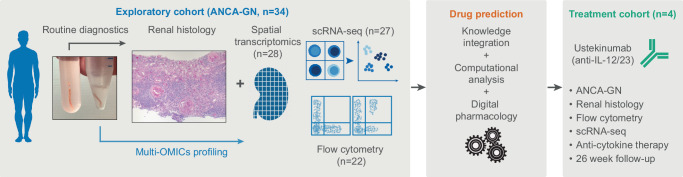
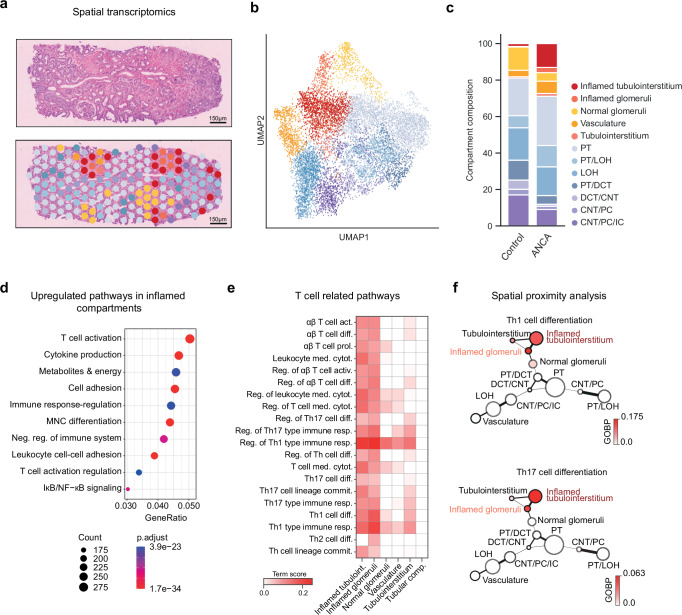
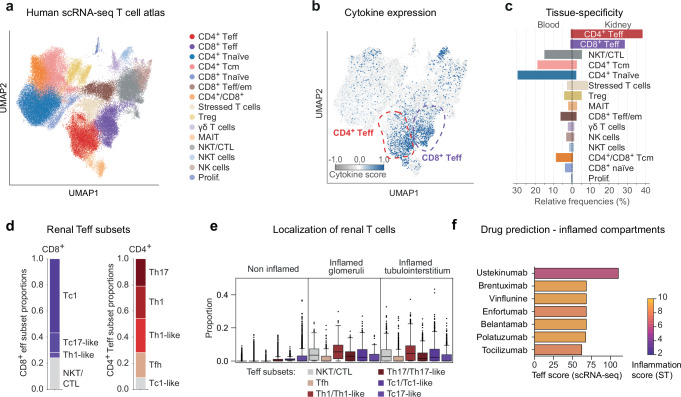
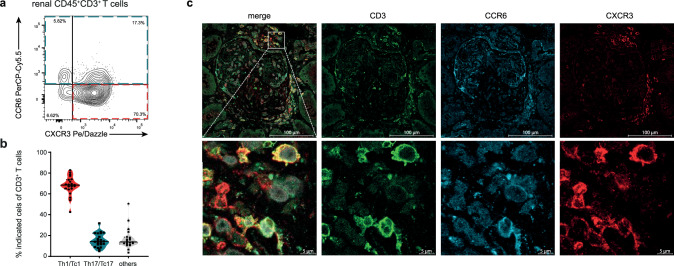
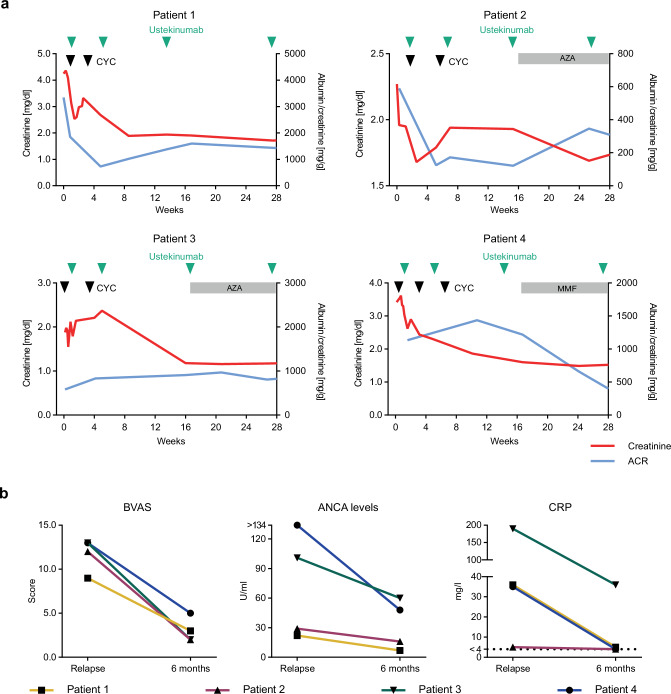
Antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis is a life-threatening autoimmune disease that often results in kidney failure caused by crescentic glomerulonephritis (GN). To date, treatment of most patients with ANCA-GN relies on non-specific immunosuppressive agents, which may have serious adverse effects and be only partially effective. Here, using spatial and single-cell transcriptome analysis, we characterize inflammatory niches in kidney samples from 34 patients with ANCA-GN and identify proinflammatory, cytokine-producing CD4+ and CD8+ T cells as a pathogenic signature. We then utilize these transcriptomic profiles for digital pharmacology and identify ustekinumab, a monoclonal antibody targeting IL-12 and IL-23, as the strongest therapeutic drug to use. Moreover, four patients with relapsing ANCA-GN are treated with ustekinumab in combination with low-dose cyclophosphamide and steroids, with ustekinumab given subcutaneously (90 mg) at weeks 0, 4, 12, and 24. Patients are followed up for 26 weeks to find this treatment well-tolerated and inducing clinical responses, including improved kidney function and Birmingham Vasculitis Activity Score, in all ANCA-GN patients. Our findings thus suggest that targeting of pathogenic T cells in ANCA-GN patients with ustekinumab might represent a potential approach and warrants further investigation in clinical trials.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Kitching, A. R. et al. ANCA-associated vasculitis. Nat. Rev. Dis. Prim.6, 71 (2020). - PubMed
-
- Kurts, C., Panzer, U., Anders, H.-J. & Rees, A. J. The immune system and kidney disease. Basic concepts and clinical implications. Nat. Rev. Immunol.13, 738–753 (2013). - PubMed
-
- Wilde, B., van Paassen, P., Witzke, O. & Tervaert, J. W. C. New pathophysiological insights and treatment of ANCA-associated vasculitis. Kidney Int.79, 599–612 (2011). - PubMed
-
- Guillevin, L. et al. Rituximab versus azathioprine for maintenance in ANCA-associated vasculitis. N. Engl. J. Med.371, 1771–1780 (2014). - PubMed
Publication types
MeSH terms
Substances
Associated data
- Actions
- Actions
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
