

Observations from the first 100 cases of intraoperative MRI - experiences, trends and short-term outcomes
- PMID: 39300452
- PMCID: PMC11411764
- DOI: 10.1186/s12893-024-02569-y
Observations from the first 100 cases of intraoperative MRI - experiences, trends and short-term outcomes
Abstract
Background: We sought to analyze, in well-defined clinical setting, the first 100 patients treated at the intraoperative MRI (iMRI) hybrid surgical theatre at our facility in a population-based setting to evaluate which pathologies are best approached with iMRI assisted surgeries, as this is not yet clearly defined.
Methods: Patients undergoing surgery in the 3T iMRI hybrid surgical theatre at our neurosurgical department between December 2017 to May 2021 were included after informed consent. Demographic, clinical, surgical, histological, radiological and outcome parameters, as well as variables related to iMRI, were retrospectively collected and analyzed. Patients were subdivided into adult and pediatric cohorts.
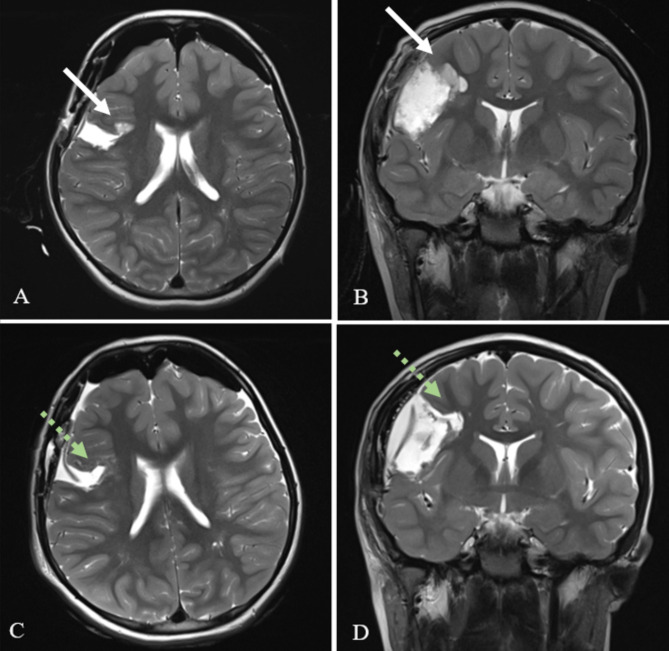
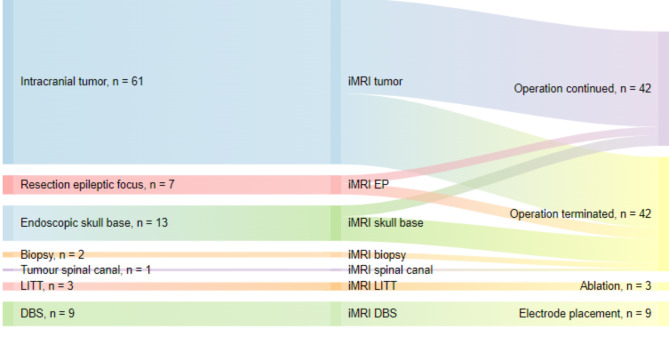
Results: Various neurosurgical procedures were performed; resection of tumors and epileptic foci, endoscopic skull base procedures including pituitary lesions, deep brain stimulation (DBS) and laser interstitial thermal therapy (LITT). In total, 41 patients were pediatric. An iMRI scan was carried out in 96% of cases and led to continuation of surgery in 50% of cases, mainly due to visualized remaining pathological tissue (95.2%). Median time to iMRI from intubation was 280 min and median total duration of surgery was 445 min. The majority of patients experienced no postoperative complications (70%), 13 patients suffered permanent postoperative deficits, predominantly visual.
Conclusion: Herein, we demonstrate the first 100 patients undergoing neurosurgery aided by iMRI at our facility since introduction. Indications for surgery differed between pediatric and adult patients. The iMRI was utilized for tumor surgeries, particularly adult low-grade gliomas and pediatric tumors, as well as for epilepsy surgery and DBS. In this heterogenous population, iMRI led to continuation of surgery in 50%. To establish the benefit in maximizing the extent of resection in these brain pathologies future studies are recommended.
Clinical trial number: Not applicable.
Keywords: Brain tumors; Deep brain stimulation; MRI scan; Neurosurgery.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Coburger J, Scheuerle A, Thal DR, Engelke J, Hlavac M, Wirtz CR, et al. Linear array ultrasound in low-grade glioma surgery: histology-based assessment of accuracy in comparison to conventional intraoperative ultrasound and intraoperative MRI. Acta Neurochir (Wien). 2015;157(2):195–206. - PubMed
-
- Scatliff JH, Morris PJ. From Roentgen to magnetic resonance imaging: the history of medical imaging. N C Med J. 2014;75(2):111–3. - PubMed
-
- Dwivedi R, Ramanujam B, Chandra PS, Sapra S, Gulati S, Kalaivani M, et al. Surgery for drug-resistant Epilepsy in Children. N Engl J Med. 2017;377(17):1639–47. - PubMed
-
- Choi SA, Kim SY, Kim H, Kim WJ, Kim H, Hwang H, et al. Surgical outcome and predictive factors of epilepsy surgery in pediatric isolated focal cortical dysplasia. Epilepsy Res. 2018;139:54–9. - PubMed
-
- Rogers CM, Jones PS, Weinberg JS. Intraoperative MRI for brain tumors. J Neurooncol. 2021;151(3):479–90. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
