

Telemedicine for the provision of medication abortion to pregnant people at up to twelve weeks of pregnancy: a systematic literature review and meta-analysis
- PMID: 39300581
- PMCID: PMC11414230
- DOI: 10.1186/s12978-024-01864-4
Telemedicine for the provision of medication abortion to pregnant people at up to twelve weeks of pregnancy: a systematic literature review and meta-analysis
Abstract
Background: Telemedicine represents an important strategy to facilitate access to medication abortion (MAB) procedures, reduces distance barriers and expands coverage to underserved communities. The aim is evaluating the self-managed MAB (provided through telemedicine as the sole intervention or in comparison to in-person care) in pregnant people at up to 12 weeks of pregnancy.
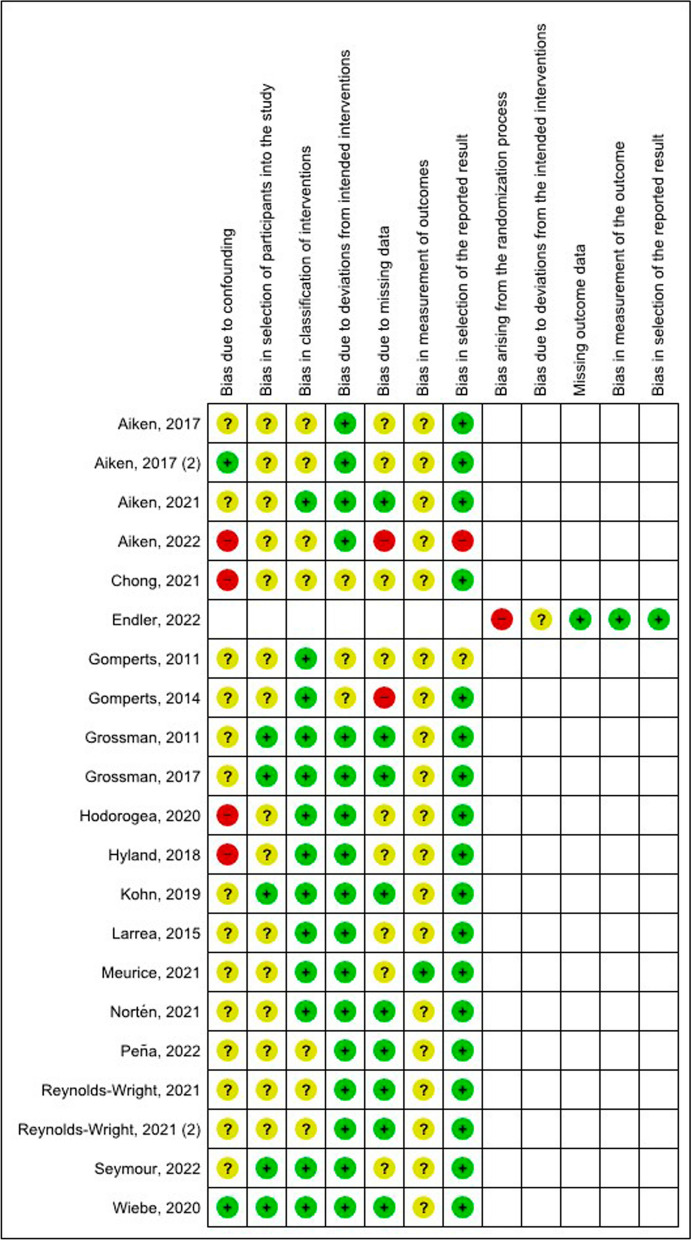
Methods: A literature search was conducted using electronic databases: MEDLINE, Embase, Cochrane (Central Register of Controlled Trials and Database of Systematic Reviews), LILACS, SciELO, and Google Scholar. The search was based on the Population, Intervention, Comparison, Outcome, and Study Design (PICOS) framework, and was not restricted to any years of publication, and studies could be published in English or Spanish. Study screening and selection, risk of bias assessment, and data extraction were performed by peer reviewers. Risk of bias was evaluated with RoB 2.0 and ROBIS-I. A narrative and descriptive synthesis of the results was conducted. Meta-analyses with random-effects models were performed using Review Manager version 5.4 to calculate pooled risk differences, along with their individual 95% confidence intervals. The rate of evidence certainty was based on GRADE recommendations.
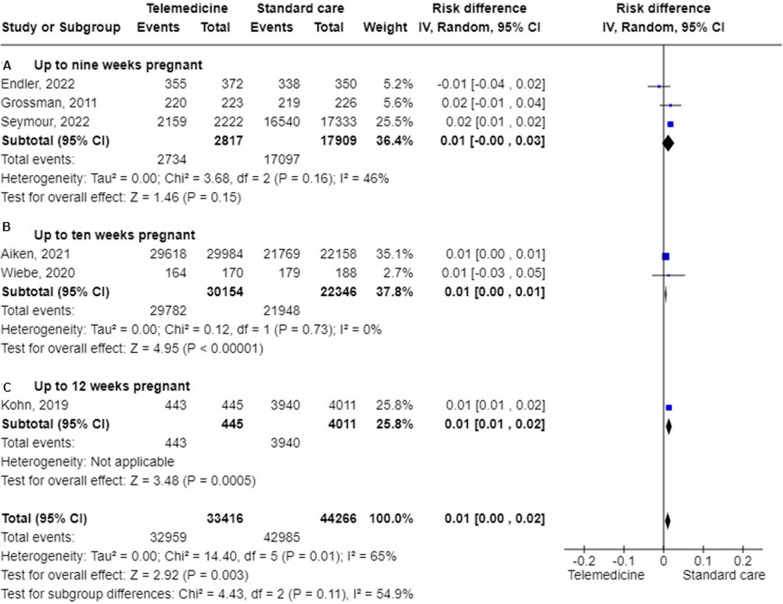
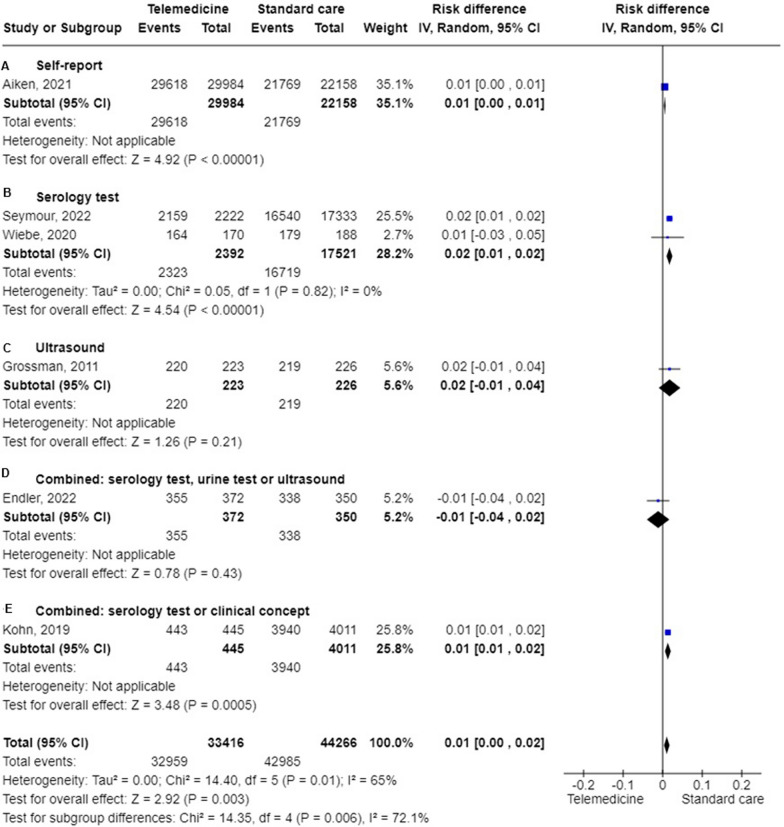
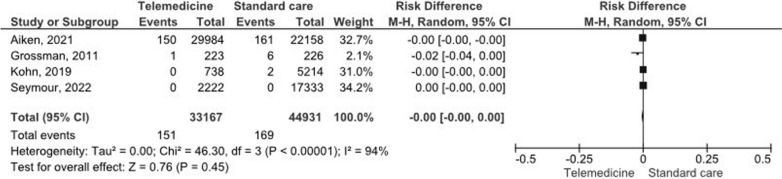
Results: 21 articles published between 2011 and 2022 met the inclusion criteria. Among them, 20 were observational studies, and 1 was a randomized clinical trial. Regarding the risk of bias, 5 studies had a serious risk, 15 had a moderate risk, and 1 had an undetermined risk. In terms of the type of intervention, 7 compared telemedicine to standard care. The meta-analysis of effectiveness revealed no statistically significant differences between the two modalities of care (RD = 0.01; 95%CI 0.00, 0.02). Our meta-analyses show that there were no significant differences in the occurrence of adverse events or in patient satisfaction when comparing the two methods of healthcare delivery.
Conclusion: Telemedicine is an effective and viable alternative for MAB, similar to standard care. The occurrence of complications was low in both forms of healthcare delivery. Telemedicine services are an opportunity to expand access to safe abortion services.
Keywords: Acceptability; Adverse effects; Effectiveness; First trimester; Medication abortion; Meta-analysis; Satisfaction; Standard care; Systematic review; Telemedicine.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




Similar articles
-
Follow-up strategies to confirm the success of medical abortion of pregnancies up to 10 weeks' gestation: a systematic review with meta-analyses.Am J Obstet Gynecol. 2020 Jun;222(6):551-563.e13. doi: 10.1016/j.ajog.2019.11.1244. Epub 2019 Nov 9. Am J Obstet Gynecol. 2020. PMID: 31715147
-
Medical abortion offered in pharmacy versus clinic-based settings.Cochrane Database Syst Rev. 2021 Jun 11;6(6):CD013566. doi: 10.1002/14651858.CD013566.pub2. Cochrane Database Syst Rev. 2021. PMID: 34114643 Free PMC article.
-
Effectiveness and safety of medication abortion via telemedicine versus in-person: A cohort of pregnant people in Colombia.Contraception. 2024 Oct;138:110514. doi: 10.1016/j.contraception.2024.110514. Epub 2024 Jun 13. Contraception. 2024. PMID: 38879070
-
Effectiveness, safety and acceptability of self-assessment of the outcome of first-trimester medical abortion: a systematic review and meta-analysis.BJOG. 2019 Dec;126(13):1536-1544. doi: 10.1111/1471-0528.15922. Epub 2019 Sep 18. BJOG. 2019. PMID: 31471989
-
Innovation through telemedicine to improve medication abortion access in primary health centers: findings from a pilot study in Musanze District, Rwanda.BMC Public Health. 2025 May 7;25(1):1681. doi: 10.1186/s12889-025-22629-z. BMC Public Health. 2025. PMID: 40335961 Free PMC article.
References
-
- World Health Organization. Safe abortion: technical and policy guidance for health systems, 2nd ed. [Internet]. 2° Edición. 2012. https://apps.who.int/iris/handle/10665/77079 - PubMed
-
- World Health Organization. Abortion care guideline: executive summary. In 2022. http://apps.who.int/bookorders. - PubMed
-
- Singh S, Remez L, Sedgh G, Kwok L, Onda T. Abortion Worldwide 2017: Uneven Progress and Unequal Access [Internet]. 2018. https://www.guttmacher.org/report/abortion-worldwide-2017
-
- Warriner I, Shah I. Preventing unsafe abortion and its consequences: priorities for research and action. New York: Guttmacher Institute [Internet]. 2006 [cited 2023 May 16]; https://www.guttmacher.org/sites/default/files/report_pdf/preventingunsa...
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
