

Reconstructive surgical therapy of peri-implant defects with ribose cross-linked collagen matrix and crosslinked hyaluronic acid - a prospective case series
- PMID: 39302523
- PMCID: PMC11415415
- DOI: 10.1007/s00784-024-05942-6
Reconstructive surgical therapy of peri-implant defects with ribose cross-linked collagen matrix and crosslinked hyaluronic acid - a prospective case series
Abstract
Objective: To investigate the efficacy of ribose-crosslinked collagen (RCLC) matrices functionalized by crosslinked hyaluronic acid (xHya) for reconstructive treatment of class I and III (b-c) peri-implantitis lesions in a transmucosal healing mode.
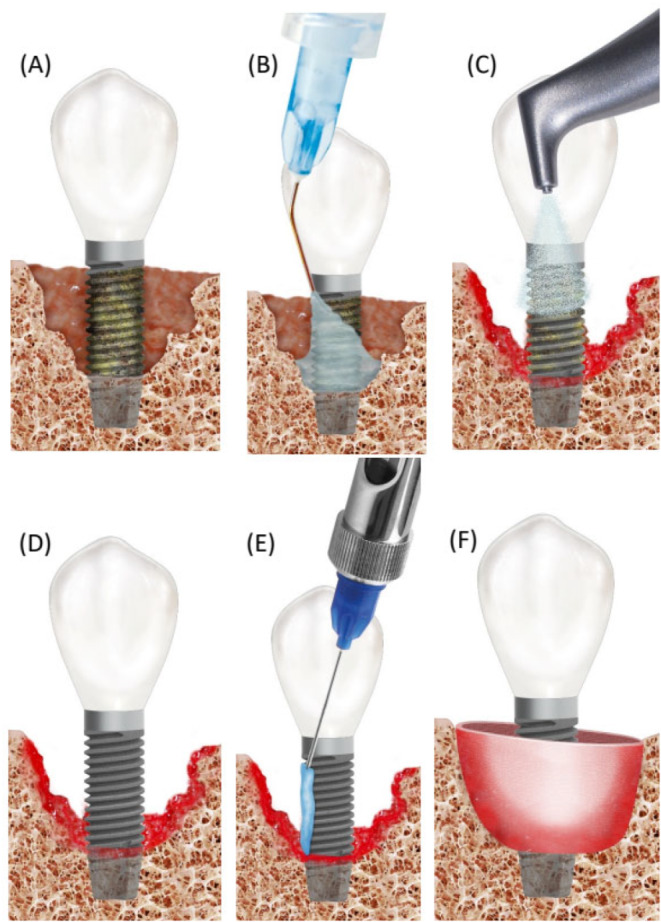
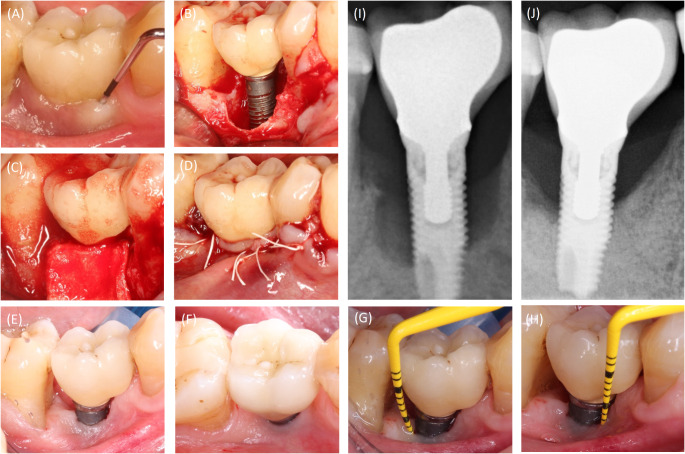
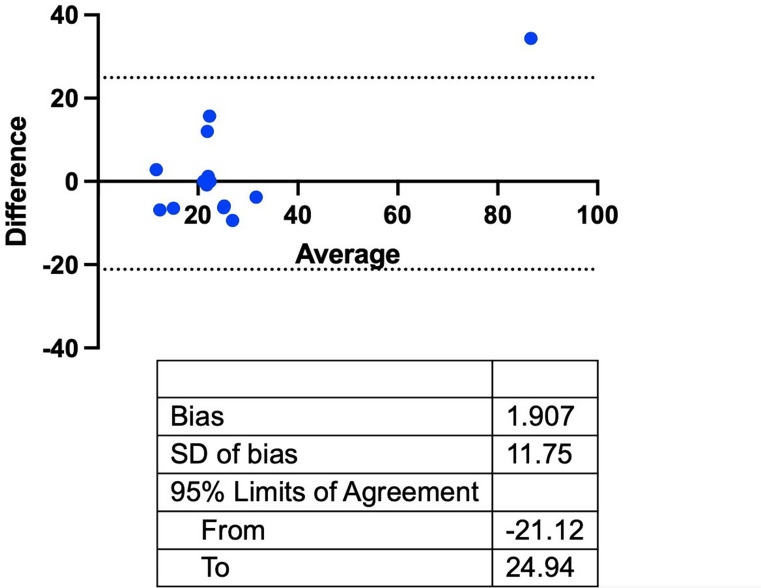
Materials and methods: Thirteen patients presenting with 15 implants were included in this prospective case series. Upon flap reflection, the implants were thoroughly decontaminated employing glycine powder air polishing and adjunctive sodium hypochlorite. For defect augmentation, xHyA was administered to the bony defect walls, exposed implant surfaces, and the RCLC matrix before defect grafting. The full-thickness flap was readapted and sutured around the implant neck for transmucosal healing. Baseline and respective values at the 12 months post-op evaluation were recorded for the clinical parameters peri-implant probing depth (PPD), buccal soft tissue dehiscence (BSTD) and bleeding on probing (BoP). Furthermore, two independent investigators analyzed radiographic changes in the defect area. The mean changes for all variables were analyzed with a paired t-test.
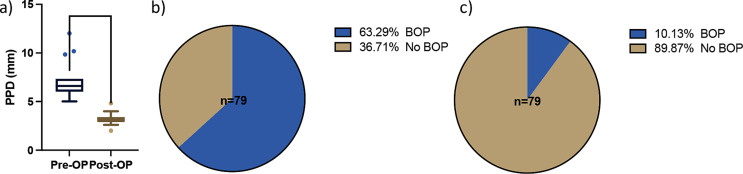
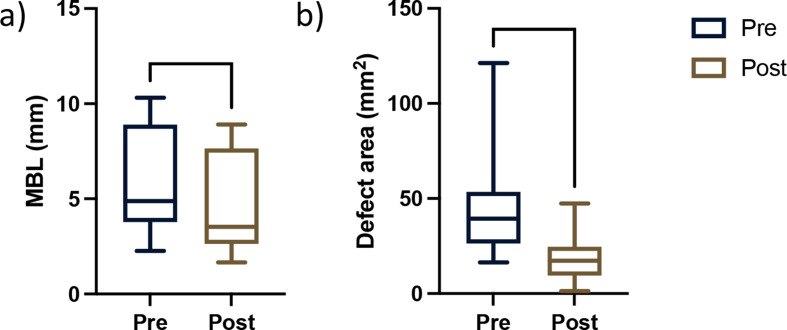
Results: The initial mean PPD was 7.2 ± 1.9 mm, and BoP was present in 63% of sites. After 12 months, PPD at the latest visit was 3.2 ± 0.66 mm, which amounted to a respective 3.9 ± 1.85 mm reduction, while the BoP frequency dropped to 10% at all sites. Radiographic bone fill was accomplished for 62.8% of the former defect area, accompanied by a mean MBL gain of 1.02 mm around the treated implants (all p < 0.001).
Conclusions: Within the limits of this case series, we conclude that the proposed treatment sequence substantially improved peri-implant defects and offered a simplified but predictive technique.
Clinical relevance: Reconstructive treatment approaches for peri-implantitis are effective but remain non-superior to open flap debridement. Further research on novel biomaterial combinations that may improve reconstructive treatment outcomes are warranted. Ribose-crosslinked collagen matrices biofunctionalized by hyaluronic acid used in this study yield improved clinical and radiographic peri-implant conditions after 12 months.
Keywords: Crosslinked hyaluronic acid; Decontamination; Hypochlorite/aminoacid gel; Peri-implant defect; RCLC; Reconstructive surgery; xHyA.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Clinical and radiographic outcomes of a surgical reconstructive approach in the treatment of peri-implantitis lesions: A 5-year prospective case series.Clin Oral Implants Res. 2018 Oct;29(10):1025-1037. doi: 10.1111/clr.13369. Epub 2018 Sep 28. Clin Oral Implants Res. 2018. PMID: 30267445
-
Reconstruction of Peri-implant Osseous Defects: A Multicenter Randomized Trial.J Dent Res. 2016 Jan;95(1):58-66. doi: 10.1177/0022034515610056. Epub 2015 Oct 8. J Dent Res. 2016. PMID: 26450511 Clinical Trial.
-
Reconstructive surgical therapy of peri-implantitis: A multicenter randomized controlled clinical trial.Clin Oral Implants Res. 2022 Sep;33(9):921-944. doi: 10.1111/clr.13972. Epub 2022 Jul 26. Clin Oral Implants Res. 2022. PMID: 35804491 Free PMC article. Clinical Trial.
-
Surgical Reconstructive Therapy for the Management of Peri-implantitis: An AAP/AO Systematic Review and Network Meta-analysis.Int J Oral Maxillofac Implants. 2025 Jun 6;(4):1-48. doi: 10.11607/jomi.2025suppl1. Int J Oral Maxillofac Implants. 2025. PMID: 40476895
-
Efficacy of reconstructive surgical therapy at peri-implantitis-related bone defects. A systematic review and meta-analysis.J Clin Periodontol. 2019 Jun;46 Suppl 21:340-356. doi: 10.1111/jcpe.13070. J Clin Periodontol. 2019. PMID: 30667523
Cited by
-
Fluid-Dynamic Crestal Sinus Floor Elevation in Atrophic Posterior Maxilla Implant Rehabilitation with Hyaluronic Acid: A Prospective Study.Materials (Basel). 2025 May 12;18(10):2230. doi: 10.3390/ma18102230. Materials (Basel). 2025. PMID: 40428967 Free PMC article.
-
Organoid-Like Neurovascular Spheroids Promote the Recovery of Hypoxic-Ischemic Skin Flaps Through the Activation of Autophagy.Adv Healthc Mater. 2025 Jun;14(15):e2405154. doi: 10.1002/adhm.202405154. Epub 2025 Apr 16. Adv Healthc Mater. 2025. PMID: 40237031 Free PMC article.
-
Role of hyaluronic acid in the treatment of peri-implant diseases: results of a meta-analysis.Front Oral Health. 2025 May 1;6:1564599. doi: 10.3389/froh.2025.1564599. eCollection 2025. Front Oral Health. 2025. PMID: 40376205 Free PMC article.
References
-
- Schwarz F, Derks J, Monje A, Wang HL (2018) Peri-implantitis. J Clin Periodontol 45:S246–S266 - PubMed
-
- Herrera D, Berglundh T, Schwarz F et al (2023) Prevention and treatment of peri-implant diseases—the EFP S3 level clinical practice guideline. J Clin Periodontol 50:4–76 - PubMed
-
- Lindhe J, Meyle J, Periodontology, GDotEWo (2008) Peri-implant diseases: consensus report of the sixth European workshop on periodontology. J Clin Periodontol 35:282–285 - PubMed
-
- Claffey N, Clarke E, Polyzois I, Renvert S (2008) Surgical treatment of peri-implantitis. J Clin Periodontol 35(8 Suppl):316–332 - PubMed
-
- Renvert S, Roos-Jansåker AM, Claffey N (2008) Non‐surgical treatment of Peri‐implant mucositis and peri‐implantitis: a literature review. J Clin Periodontol 35:305–315 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
