

Quality control of elbow joint radiography using a YOLOv8-based artificial intelligence technology
- PMID: 39302546
- PMCID: PMC11415556
- DOI: 10.1186/s41747-024-00504-7
Quality control of elbow joint radiography using a YOLOv8-based artificial intelligence technology
Abstract
Background: To explore an artificial intelligence (AI) technology employing YOLOv8 for quality control (QC) on elbow joint radiographs.
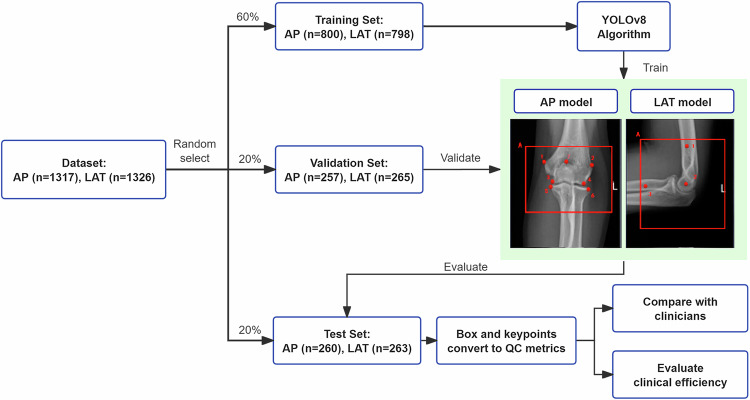
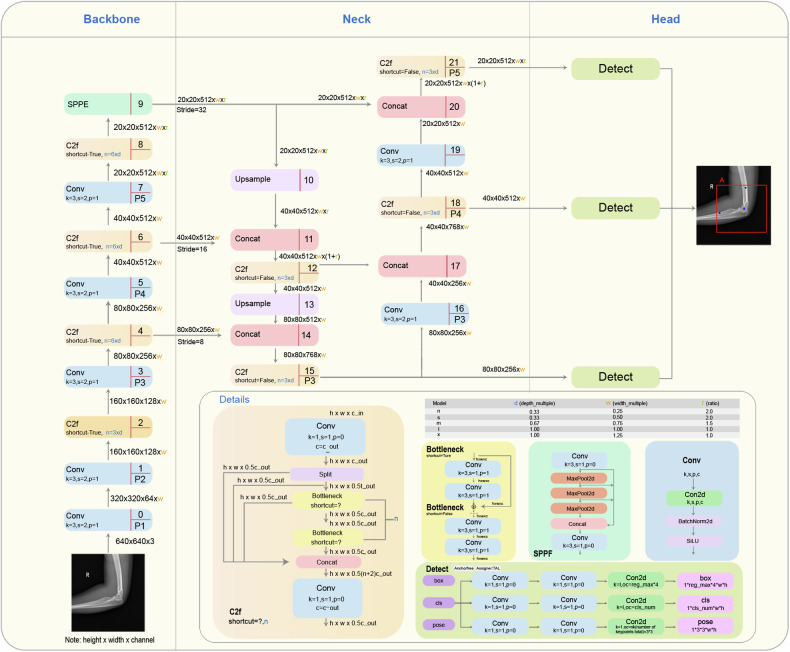
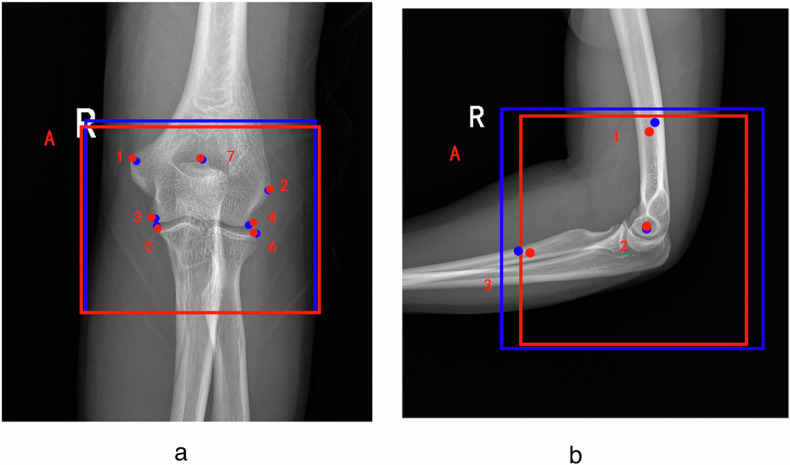
Methods: From January 2022 to August 2023, 2643 consecutive elbow radiographs were collected and randomly assigned to the training, validation, and test sets in a 6:2:2 ratio. We proposed the anteroposterior (AP) and lateral (LAT) models to identify target detection boxes and key points on elbow radiographs using YOLOv8. These identifications were transformed into five quality standards: (1) AP elbow positioning coordinates (XA and YA); (2) olecranon fossa positioning distance parameters (S17 and S27); (3) key points of joint space (Y3, Y4, Y5 and Y6); (4) LAT elbow positioning coordinates (X2 and Y2); and (5) flexion angle. Models were trained and validated using 2,120 radiographs. A test set of 523 radiographs was used for assessing the agreement between AI and physician and to evaluate clinical efficiency of models.
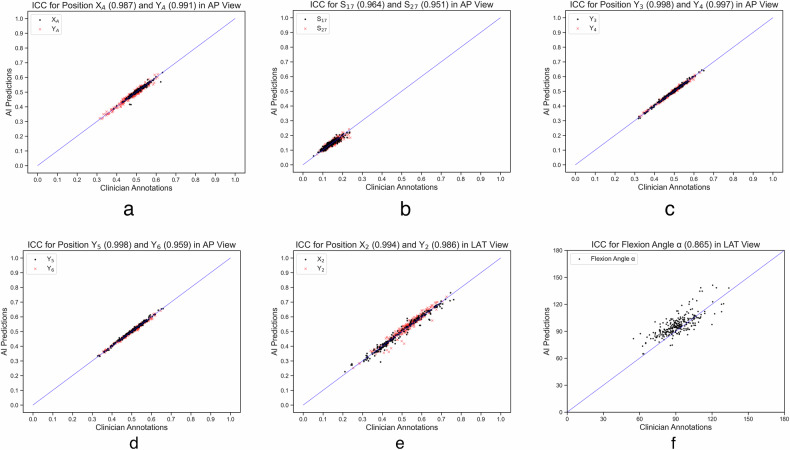
Results: The AP and LAT models demonstrated high precision, recall, and mean average precision for identifying boxes and points. AI and physicians showed high intraclass correlation coefficient (ICC) in evaluating: AP coordinates XA (0.987) and YA (0.991); olecranon fossa parameters S17 (0.964) and S27 (0.951); key points Y3 (0.998), Y4 (0.997), Y5 (0.998) and Y6 (0.959); LAT coordinates X2 (0.994) and Y2 (0.986); and flexion angle (0.865). Compared to manual methods, using AI, QC time was reduced by 43% for AP images and 45% for LAT images (p < 0.001).
Conclusion: YOLOv8-based AI technology is feasible for QC of elbow radiography with high performance.
Relevance statement: This study proposed and validated a YOLOv8-based AI model for automated quality control in elbow radiography, obtaining high efficiency in clinical settings.
Key points: QC of elbow joint radiography is important for detecting diseases. Models based on YOLOv8 are proposed and perform well in image QC. Models offer objective and efficient solutions for QC in elbow joint radiographs.
Keywords: Artificial intelligence; Deep learning; Elbow joint; Quality control; Radiography.
© 2024. The Author(s).
Conflict of interest statement
All authors declare that they have no competing interests in this study.
Figures


References
-
- Sheehan SE, Dyer GS, Sodickson AD, Patel KI, Khurana B (2013) Traumatic elbow injuries: what the orthopedic surgeon wants to know. Radiographics 33:869–888. 10.1148/rg.333125176 - PubMed
-
- Crosby NE, Greenberg JA (2014) Radiographic evaluation of the elbow. J Hand Surg Am 39:1408–1414. 10.1016/j.jhsa.2014.04.035 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials