

Hypertrophic obstructive cardiomyopathy-left ventricular outflow tract shapes and their hemodynamic influences applying CMR
- PMID: 39302632
- PMCID: PMC11561129
- DOI: 10.1007/s10554-024-03242-4
Hypertrophic obstructive cardiomyopathy-left ventricular outflow tract shapes and their hemodynamic influences applying CMR
Abstract
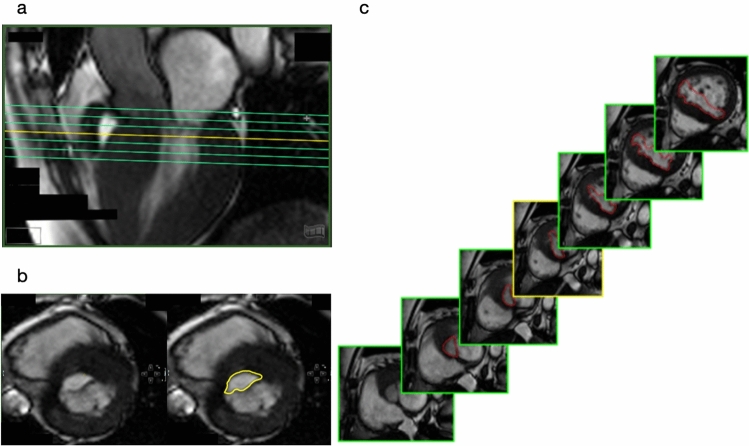
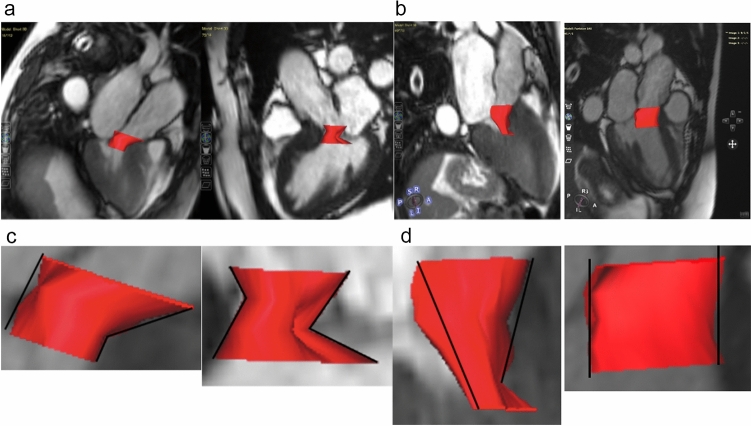
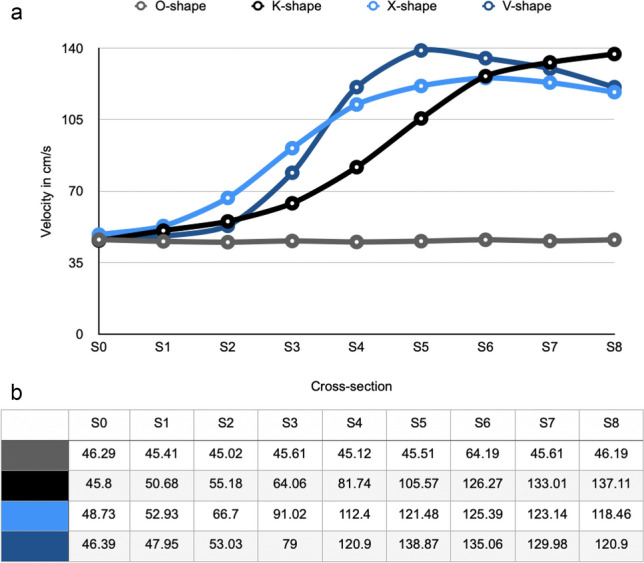
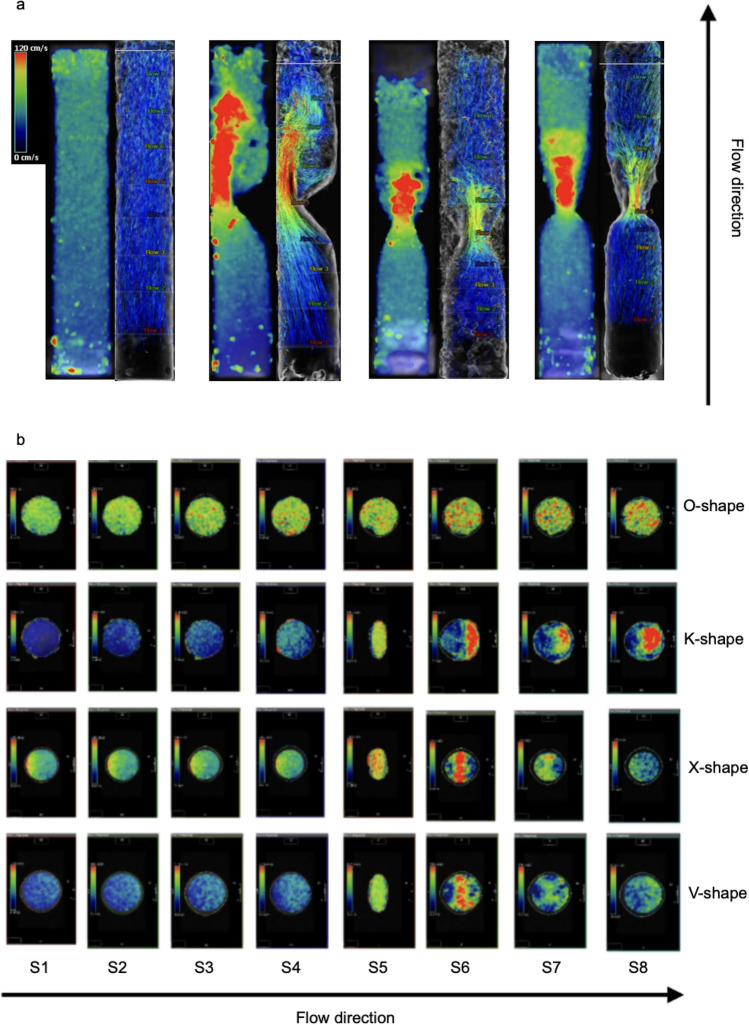
Hypertrophic cardiomyopathy (HCM) is one of the most common genetic cardiac disorders and is characterized by different phenotypes of left ventricular hypertrophy with and without obstruction. The effects of left ventricular outflow tract (LVOT) obstruction based on different anatomies may be hemodynamically relevant and influence therapeutic decision making. Cardiovascular magnetic resonance (CMR) provides anatomical information. We aimed to identify different shapes of LVOT-obstruction using Cardiovascular Magnetic Resonance (CMR). The study consisted of two parts: An in-vivo experiment for shape analysis and in-vitro part for the assessment of its hemodynamic consequences. In-vivo a 3D depiction of the LVOT was created using a 3D multi-slice reconstruction from 2D-slices (full coverage cine stack with 7 slices and a thickness of 5-6 mm with no gap) in 125 consecutive HOCM patients (age = 64.17 +/- 12.655; female n = 42). In-vitro an analysis of the LVOT regarding shape and flow behavior was conducted. For this purpose, 2D and 4D measurements were performed on 3D printed phantoms which were based on the anatomical characteristics of the in-vivo study, retrospectively. The in-vivo study identified three main shapes named K- (28.8%), X- (51.2%) and V-shape (10.4%) and a mixed one (9.6%). By analyzing the in-vitro flow measurements every shape showed an individual flow profile in relation to the maximum velocity in cm/s. Here, the V-shape showed the highest value of velocity (max. 138.87 cm/s). The X-shape was characterized by a similar profile but with lower velocity values (max. 125.39 cm/s), whereas the K-shape had an increase of the velocity without decrease (max. 137.11 cm/s). For the first time three different shapes of LVOT-obstruction could be identified. These variants seem to affect the hemodynamics in HOCM.
Keywords: Cardiovascular magnetic resonance; Hemodynamics; Hypertrophic cardiomyopathy; Hypertrophic obstructive cardiomyopathy; Left ventricular outflow obstruction; Shape analysis.
© 2024. The Author(s).
Conflict of interest statement
Figures





References
-
- Maron BJ (2018) Clinical course and management of hypertrophic cardiomyopathy. N Engl J Med 379(7):655–668 - PubMed
-
- Kizilbash AM, Heinle SK, Grayburn PA (1998) Spontaneous variability of left ventricular outflow tract gradient in hypertrophic obstructive cardiomyopathy. Circulation 97(5):461–466 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
