

Lipid profiling identifies modifiable signatures of cardiometabolic risk in children and adolescents with obesity
- PMID: 39304782
- PMCID: PMC11750701
- DOI: 10.1038/s41591-024-03279-x
Lipid profiling identifies modifiable signatures of cardiometabolic risk in children and adolescents with obesity
Abstract
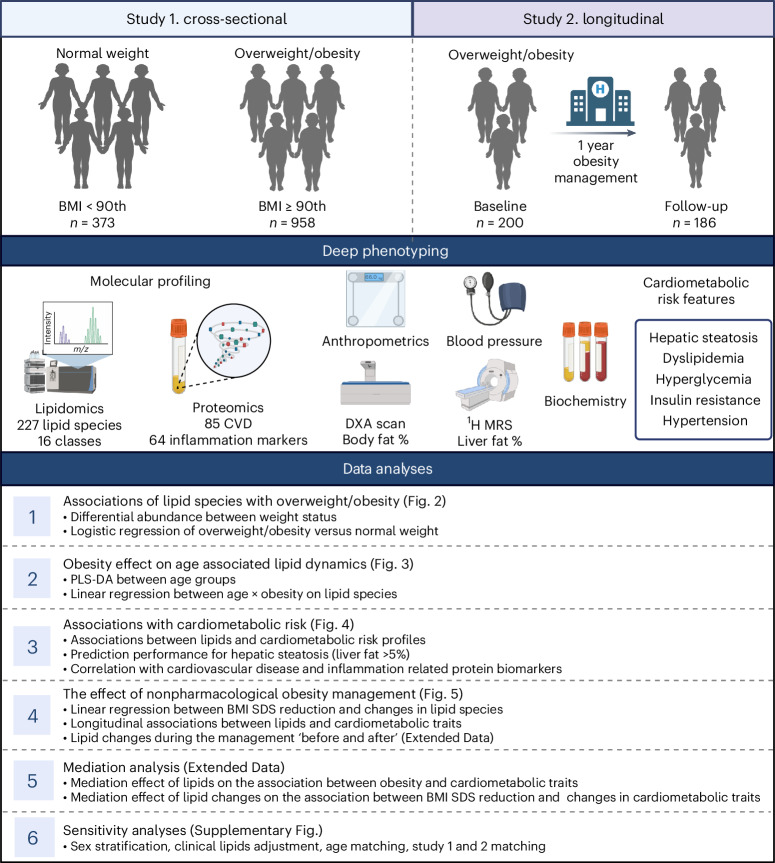
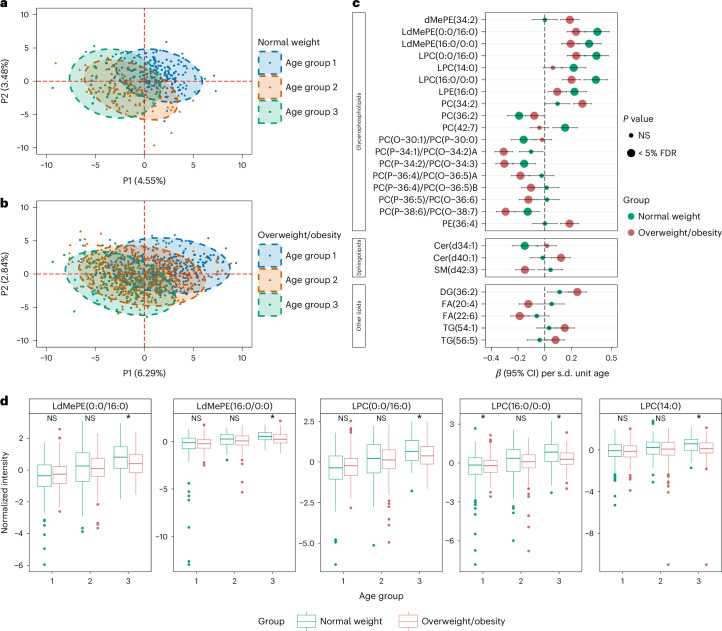
Pediatric obesity is a progressive, chronic disease that can lead to serious cardiometabolic complications. Here we investigated the peripheral lipidome in 958 children and adolescents with overweight or obesity and 373 with normal weight, in a cross-sectional study. We also implemented a family-based, personalized program to assess the effects of obesity management on 186 children and adolescents in a clinical setting. Using mass spectrometry-based lipidomics, we report an increase in ceramides, alongside a decrease in lysophospholipids and omega-3 fatty acids with obesity metabolism. Ceramides, phosphatidylethanolamines and phosphatidylinositols were associated with insulin resistance and cardiometabolic risk, whereas sphingomyelins showed inverse associations. Additionally, a panel of three lipids predicted hepatic steatosis as effectively as liver enzymes. Lipids partially mediated the association between obesity and cardiometabolic traits. The nonpharmacological management reduced levels of ceramides, phospholipids and triglycerides, indicating that lowering the degree of obesity could partially restore a healthy lipid profile in children and adolescents.
© 2024. The Author(s).
Conflict of interest statement
Competing interests: The data and paper were prepared while K.S. was employed at the Steno Diabetes Center Copenhagen. In the process of revision and publication, K.S. has started a position at Novo Nordisk. C.L.-Q. has received consultancy fees from Pfizer. C.L.-Q. has received honoraria, travel or speakers’ fees from Biogen and research funds from Pfizer and Novo Nordisk. C.L.-Q. is the director of the company BrainLogia. All of these activities are unrelated to this study. The other authors declare no competing interests.
Figures












References
-
- World Health Organization. Obesity and overweight. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (2024).
-
- Maes, H. H., Neale, M. C. & Eaves, L. J. Genetic and environmental factors in relative body weight and human adiposity. Behav. Genet.27, 325–351 (1997). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
