

Investigating the genetic basis of hereditary spastic paraplegia and cerebellar Ataxia in Pakistani families
- PMID: 39304850
- PMCID: PMC11414091
- DOI: 10.1186/s12883-024-03855-1
Investigating the genetic basis of hereditary spastic paraplegia and cerebellar Ataxia in Pakistani families
Abstract
Background: Hereditary Spastic Paraplegias (HSPs) and Hereditary Cerebellar Ataxias (HCAs) are progressive neurodegenerative disorders encompassing a spectrum of neurogenetic conditions with significant overlaps of clinical features. Spastic ataxias are a group of conditions that have features of both cerebellar ataxia and spasticity, and these conditions are frequently clinically challenging to distinguish. Accurate genetic diagnosis is crucial but challenging, particularly in resource-limited settings. This study aims to investigate the genetic basis of HSPs and HCAs in Pakistani families.
Methods: Families from Khyber Pakhtunkhwa with at least two members showing HSP or HCA phenotypes, and who had not previously been analyzed genetically, were included. Families were referred for genetic analysis by local neurologists based on the proband's clinical features and signs of a potential genetic neurodegenerative disorder. Whole Exome Sequencing (WES) and Sanger sequencing were then used to identify and validate genetic variants, and to analyze variant segregation within families to determine inheritance patterns. The mean age of onset and standard deviation were calculated to assess variability among affected individuals, and the success rate was compared with literature reports using differences in proportions and Cohen's h.
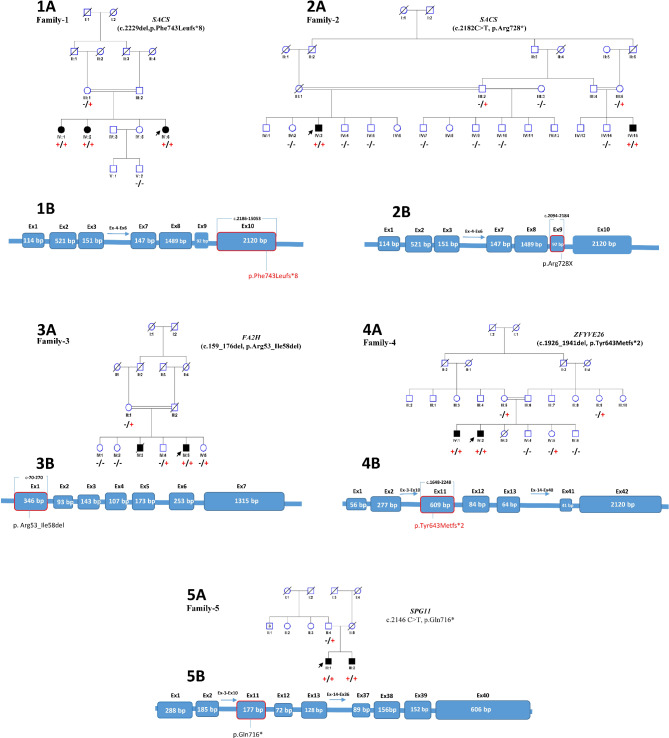
Results: Pathogenic variants associated with these conditions were identified in five of eight families, segregating according to autosomal recessive inheritance. These variants included previously reported SACS c.2182 C > T, p.(Arg728*), FA2H c.159_176del, p.(Arg53_Ile58del) and SPG11 c.2146 C > T, p.(Gln716*) variants, and two previously unreported variants in SACS c.2229del, p.(Phe743Leufs*8) and ZFYVE26 c.1926_1941del, p.(Tyr643Metfs*2). Additionally, FA2H and SPG11 variants were found to have recurrent occurrences, suggesting a potential founder effect within the Pakistani population. Onset age among affected individuals ranged from 1 to 14 years (M = 6.23, SD = 3.96). The diagnostic success rate was 62.5%, with moderate effect sizes compared to previous studies.
Conclusions: The findings of this study expand the genotypic and phenotypic spectrum of HSPs and HCAs in Pakistan and emphasize the importance of utilizing exome/genome sequencing for accurate diagnosis or support accurate differential diagnosis. This approach can improve genetic counseling and clinical management, addressing the challenges of diagnosing neurodegenerative disorders in resource-limited settings.
Keywords: Hereditary Cerebellar Ataxias; Hereditary Spastic Paraplegias; Neurodegenerative disorders; Pakistani families; Spastic ataxia.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Alonso V, Villaverde-Hueso A, Hens MJ, Morales-Piga A, Abaitua I, Posada de la Paz M. Epidemiology of hereditary ataxias in Spain: hospital discharge registry and population-based mortality study. Neuroepidemiology. 2013;41(1):13–9. 10.1159/000346275. - PubMed
-
- Erichsen AK, Koht J, Stray-Pedersen A, Abdelnoor M, Tallaksen CM. Prevalence of hereditary ataxia and spastic paraplegia in southeast Norway: a population-based study. Brain. 2009;132:1577–88. 10.1093/brain/awp056. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
