

Role of cfDNA and ctDNA to improve the risk stratification and the disease follow-up in patients with endometrial cancer: towards the clinical application
- PMID: 39304963
- PMCID: PMC11414036
- DOI: 10.1186/s13046-024-03158-w
Role of cfDNA and ctDNA to improve the risk stratification and the disease follow-up in patients with endometrial cancer: towards the clinical application
Abstract
Background: There has been a rise in endometrial cancer (EC) incidence leading to increased mortality. To counter this trend, improving the stratification of post-surgery recurrence risk and anticipating disease relapse and treatment resistance is essential. Liquid biopsy analyses offer a promising tool for these clinical challenges, though the best strategy for applying them in EC must be defined. This study was designed to determine the value of cfDNA/ctDNA monitoring in improving the clinical management of patients with localized and recurrent disease.
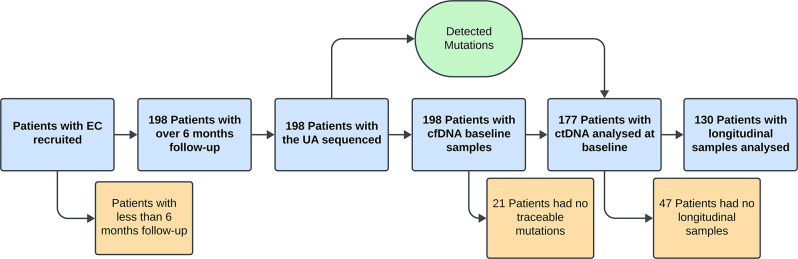
Methods: Plasma samples and uterine aspirates (UA) from 198 EC patients were collected at surgery and over time. The genetic landscape of UAs was characterized using targeted sequencing. Total cfDNA was analyzed for ctDNA presence based on the UA mutational profile.
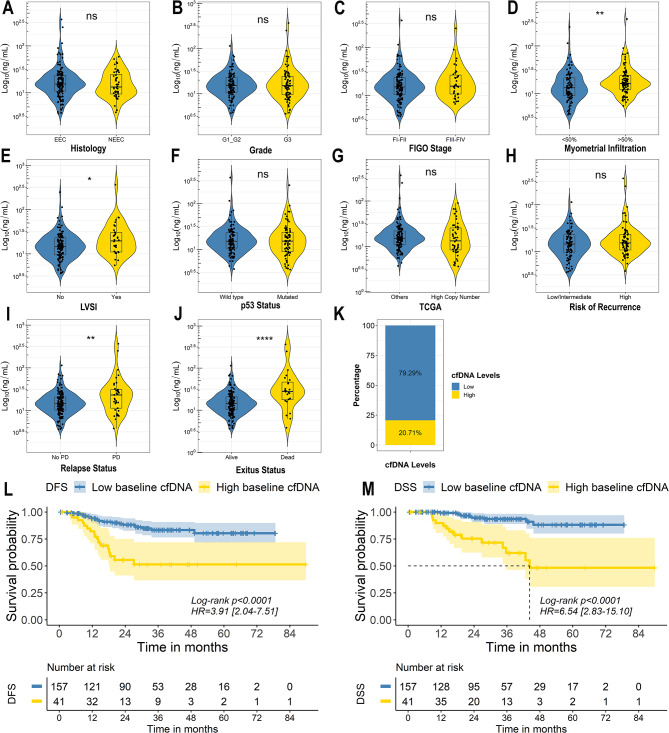
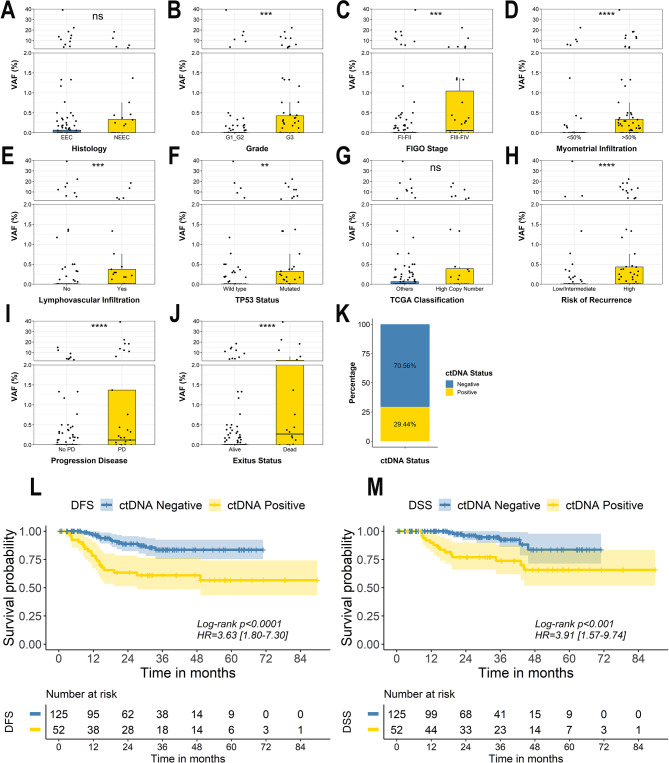
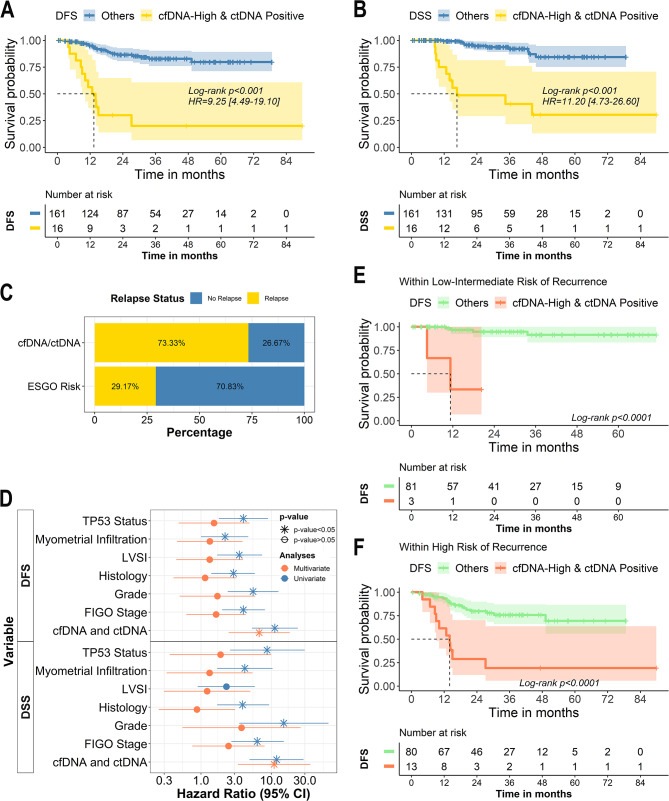
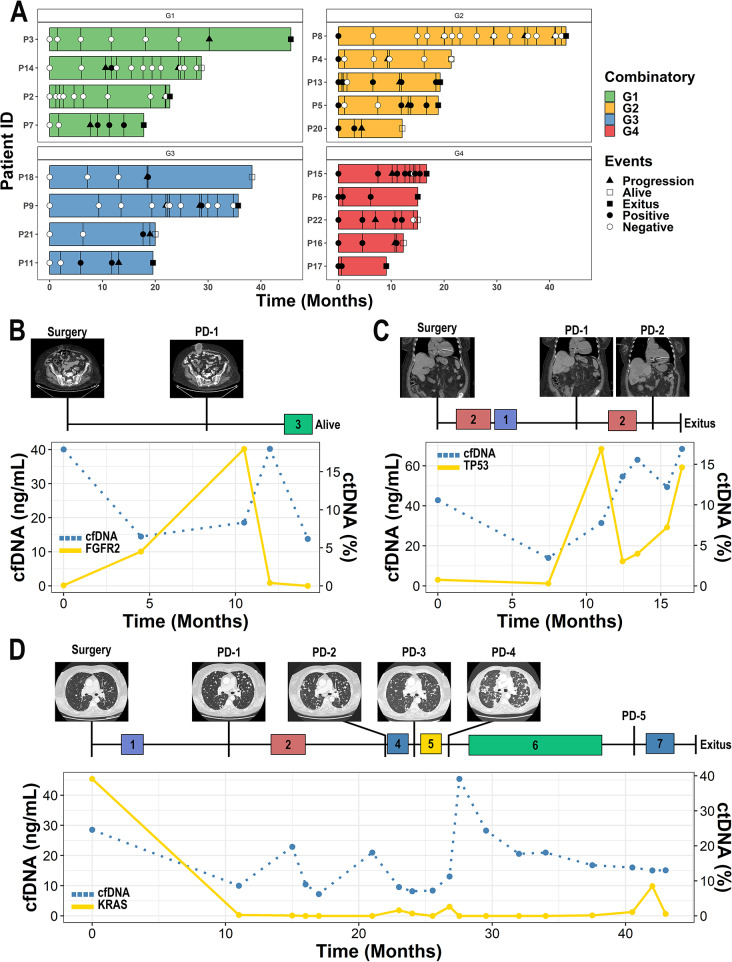
Results: High cfDNA levels and detectable ctDNA at baseline correlated with poor prognosis for DFS (p-value < 0.0001; HR = 9.25) and DSS (p-value < 0.0001; HR = 11.20). This remained clinically significant when stratifying tumors by histopathological risk factors. Of note, cfDNA/ctDNA analyses discriminated patients with early post-surgery relapse and the ctDNA kinetics served to identify patients undergoing relapse before any clinical evidence emerged.
Conclusions: This is the most comprehensive study on cfDNA/ctDNA characterization in EC, demonstrating its value in improving risk stratification and anticipating disease relapse in patients with localized disease. CtDNA kinetics assessment complements current strategies to monitor the disease evolution and the treatment response. Therefore, implementing cfDNA/ctDNA monitoring in clinical routines offers a unique opportunity to improve EC management.
Translational relevance: The study demonstrates that high levels of cfDNA and detectable ctDNA at baseline are strong indicators of poor prognosis. This enables more accurate risk stratification beyond traditional histopathological factors, allowing clinicians to identify high-risk patients who may benefit from more aggressive treatment and closer monitoring. Moreover, longitudinal analysis of cfDNA/ctDNA can detect disease recurrence months before clinical symptoms or imaging evidence appear. This early warning system offers a significant advantage in clinical practice, providing a window of opportunity for early intervention and potentially improving patient outcomes.
Keywords: Blood biomarkers; Endometrial cancer; Liquid Biopsy; Prognostic biomarkers; Tumour kinetics.
© 2024. The Author(s).
Conflict of interest statement
Authors declare no conflict of interest.
Figures
References
MeSH terms
Substances
Grants and funding
- PI20/00969/Instituto de Salud Carlos III
- PI20/01566/Instituto de Salud Carlos III
- PI21/00990/Instituto de Salud Carlos III
- AC21_2/00020/Instituto de Salud Carlos III
- Miguel Servet (CP20/00119)/Instituto de Salud Carlos III
- Miguel Servet (CP22/00147)/Instituto de Salud Carlos III
- Juan Rodés (JR21/00019)/Instituto de Salud Carlos III
- PID2022-136854OB-I00/Ministerio de Ciencia e Innovación
- CB16/12/00328/Centro de Investigación Biomédica en Red de Cáncer
- CB16/12/00295/Centro de Investigación Biomédica en Red de Cáncer
- FCAECC, GCTRA1804MATI/Fundación Científica Asociación Española Contra el Cáncer
- FCAECC-postdoctoral (PI21/00990)/Fundación Científica Asociación Española Contra el Cáncer
- IN607D2021/05/Xunta de Galicia
- IDIS-predoctoral grant/Fundación Instituto de Investigación Sanitaria de Santiago de Compostela
