

Multi-marker analysis of circulating tumor cells in localized intermediate/high-risk and metastatic prostate cancer
- PMID: 39305397
- PMCID: PMC11607046
- DOI: 10.1007/s10585-024-10313-2
Multi-marker analysis of circulating tumor cells in localized intermediate/high-risk and metastatic prostate cancer
Abstract
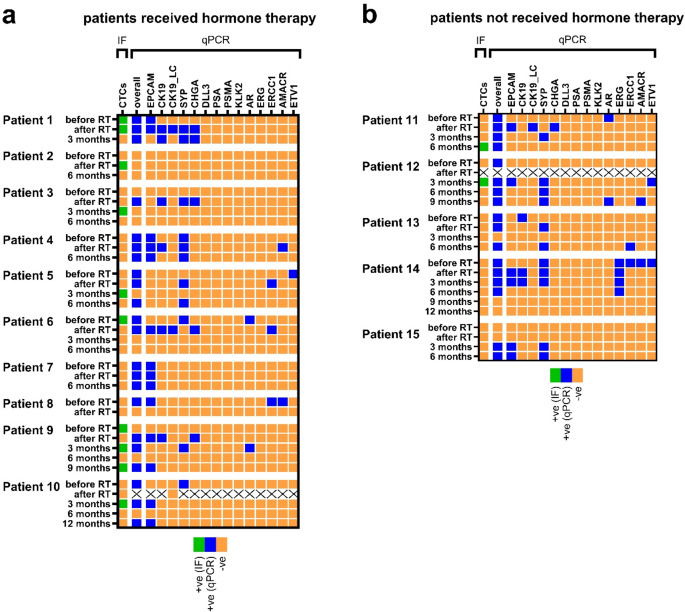
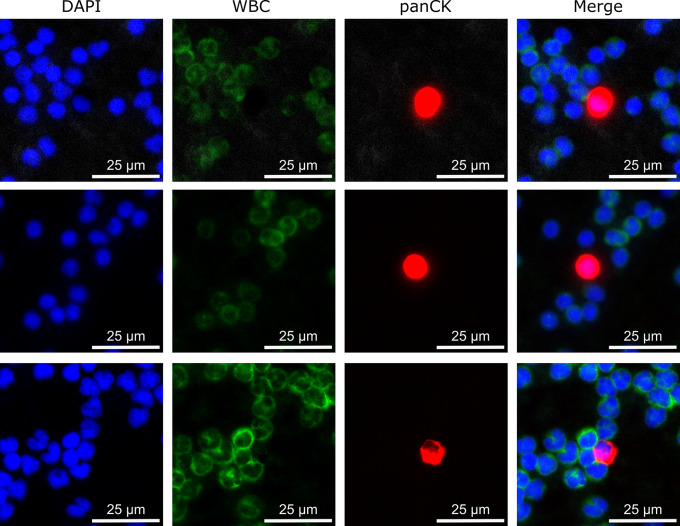
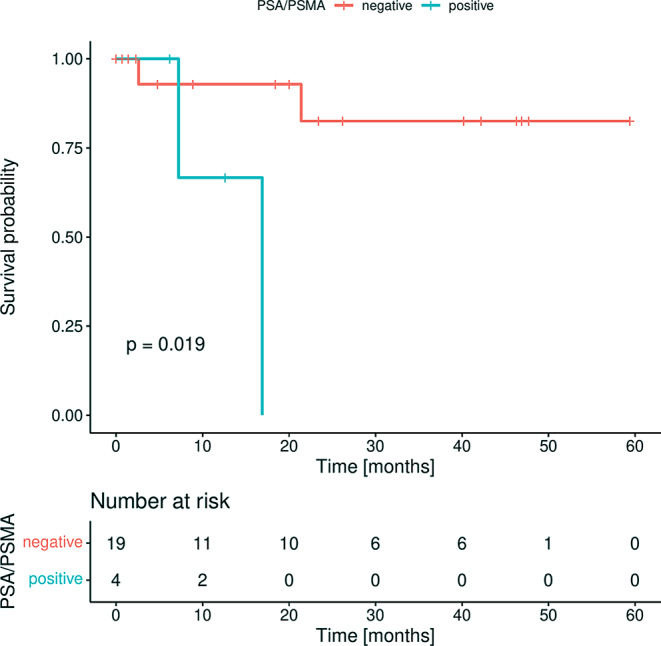
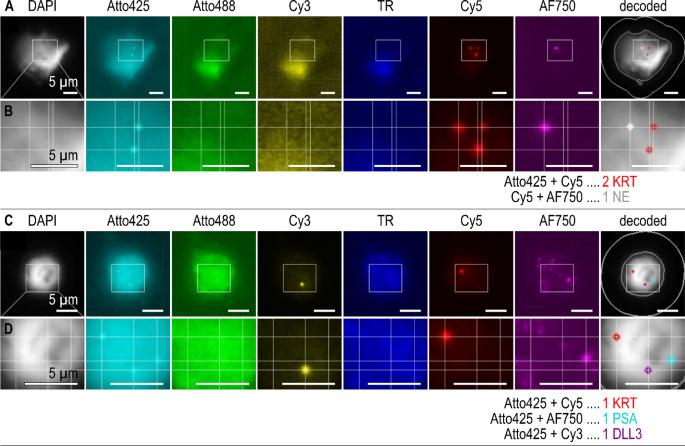
Circulating tumor cells (CTCs) are an established prognostic marker in metastatic prostate cancer (PrC) but have received little attention in localized high-risk disease. Peripheral blood was obtained from patients with early intermediate and high-risk PrC (n = 15) at baseline, after radiotherapy, and during follow-up, as well as from metastatic PrC patients (n = 23). CTCs were enriched using the microfluidic Parsortix® technology. CTC-related marker were quantified with qPCR and RNA in-situ hybridization (ISH). Positivity and associations to clinical parameters were assessed using McNemar test, Fisher Exact test or log-rank test. The overall positivity was high in both cohorts (87.0% metastatic vs. 66.7% early at baseline). A high concordance of qPCR and RNA ISH was achieved. In metastatic PrC, PSA and PSMA were prognostic for shorter overall survival. In early PrC patients, an increase of positive transcripts per blood sample was observed from before to after radiation therapy, while a decrease of positive markers was observed during follow-up. CTC analysis using the investigated qPCR marker panel serves as tool for achieving high detection rates of PrC patient samples even in localized disease. RNA ISH offers the advantage of confirming these markers at the single cell level. Employing the clinically relevant marker PSMA, our CTC approach can be used for diagnostic purposes to screen patients profiting from PSMA-directed PET-CT or PSMA-targeted therapy.
Keywords: Circulating tumor cells; Gene expression; Liquid biopsy; Parsortix; Prostate cancer; qPCR.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interest: The authors have no competing interest to declare.
Figures

References
-
- ECIS - European Cancer Information System European Union https://ecis.jrc.ec.europa.eu 20.7.2023
-
- American Cancer Society Cancer Statistics Center. http://cancerstatisticscenter.cancer.org/ 28.07.2023
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
