

A specific serum lipid signature characterizes patients with glycogen storage disease type Ia
- PMID: 39306041
- PMCID: PMC11526085
- DOI: 10.1016/j.jlr.2024.100651
A specific serum lipid signature characterizes patients with glycogen storage disease type Ia
Abstract
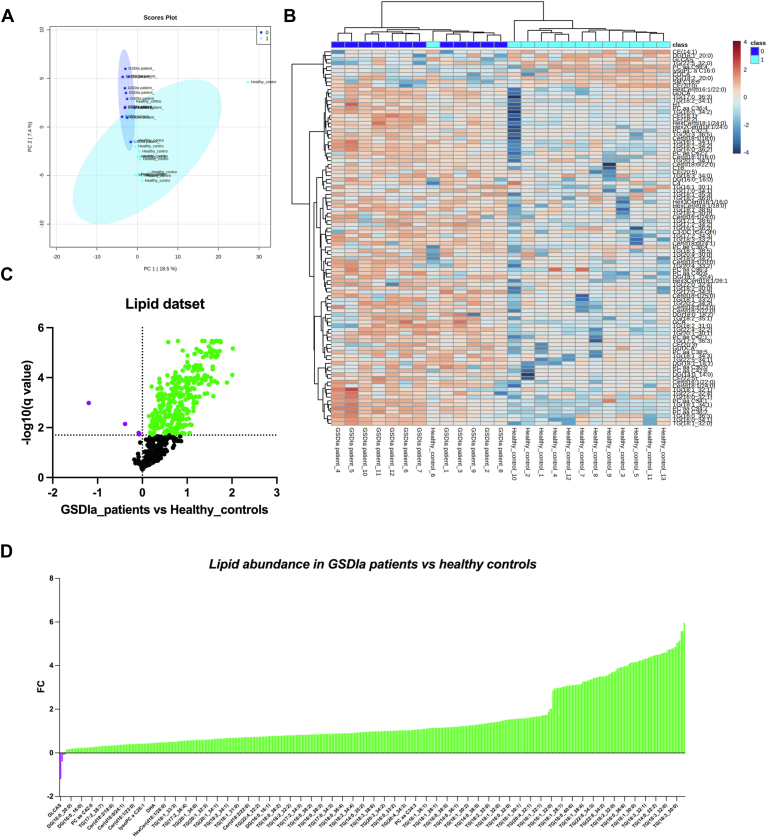
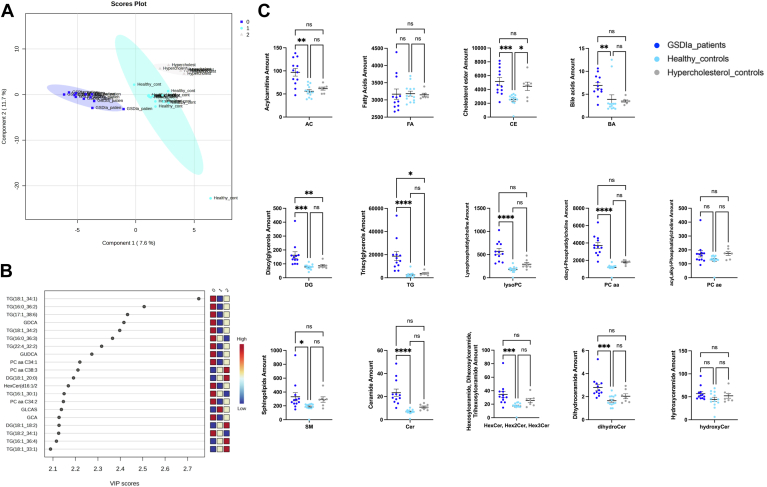
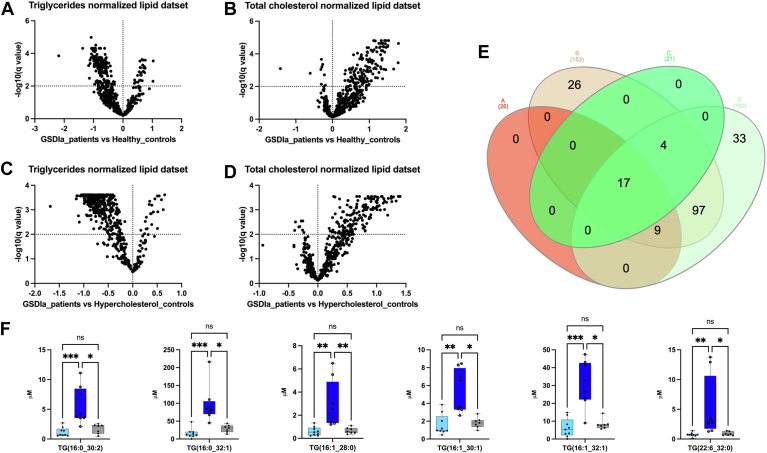
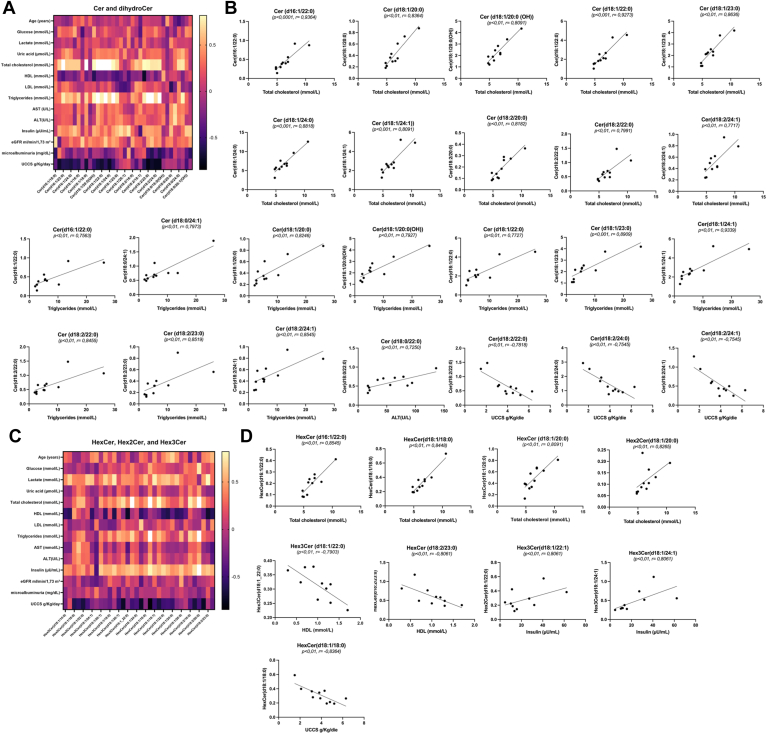
Glycogen storage disease type Ia (GSDIa) is a rare, inherited glucose-6-phosphatase-α (G6Pase-α) deficiency-induced carbohydrate metabolism disorder. Although hyperlipidemia is a hallmark of GSDI, the extent of lipid metabolism disruption remains incompletely understood. Lipidomic analysis was performed to characterize the serum lipidome in patients with GSDIa, by including age- and sex-matched healthy controls and age-matched hypercholesterolemic controls. Metabolic control and dietary information biochemical markers were obtained from patients with GSDIa. Patients with GSDIa showed higher total serum lysophosphatidylcholine (Fold Change, (FC) 2.2, P < 0.0001), acyl-acyl-phosphatidylcholine (FC 2.1, P < 0.0001), and ceramide (FC 2.4, P < 0.0001) levels and bile acid (FC 0.7, P < 0.001), acylcarnitines (FC 0.7, P < 0.001), and cholesterol esters (FC 1.0, P < 0.001) than those of healthy controls, and higher di- (FC 1.1, P < 0.0001; FC 0.9, P < 0.01) and triacylglycerol (FC 6.3, P < 0.0001; FC 3.9, P < 0.01) levels than those of healthy controls and hypercholesterolemic subjects. Both total cholesterol and triglyceride values correlated with Cer (d16:1/22:0), Cer (d18:1/20:0), Cer (d18:1/20:0(OH)), Cer (d18:1/22:0), Cer (d18:1/23:0), Cer (d18:1/24:1), Cer (d18:2/22:0), Cer (d18:2/24:1). Total cholesterol also correlated with Cer (d18:1/24:0), Cer (d18:2/20:0), HexCer (d16:1/22:0), HexCer (d18:1/18:0), and Hex2Cer (d18:1/20:0). Triglyceridelevels correlated with Cer (d18:0/24:1). Alanine aminotransferase values correlated with Cer (d18:0/22:0), insulin with Cer (d18:1/22:1) and Cer (d18:1/24:1), and HDL with hexosylceramide (HexCer) (d18:2/23:0). These results expand on the currently known involvement of lipid metabolism in GSDIa. Circulating Cer may allow for refined dietary assessment compared with traditional biomarkers. Because specific lipid species are relatively easy to assess, they represent potential novel biomarkers of GSDIa.
Keywords: bile acids; ceramides; hyperlipidemia; lysophosphatidylcholine; serum lipidome.
Copyright © 2024 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest The authors declare that they have no conflicts of interest with the contents of this article.
Figures
References
-
- Kishnani P.S., Austin S.L., Abdenur J.E., Arn P., Bali D.S., Boney A., et al. Diagnosis and management of glycogen storage disease type I: a practice guideline of the American College of Medical Genetics and Genomics. Genet. Med. 2014;16:e1–e29. - PubMed
-
- Rossi A., Hoogeveen I.J., Lubout C.M., de Boer F., Fokkert-Wilts M.J., Rodenburg I.L., et al. A generic emergency protocol for patients with inborn errors of metabolism causing fasting intolerance: a retrospective, single-center study and the generation of www.emergencyprotocol.net. J. Inherit. Metab. Dis. 2021;44:1124–1135. - PMC - PubMed
-
- Franco L.M., Krishnamurthy V., Bali D., Weinstein D.A., Arn P., Clary B., et al. Hepatocellular carcinoma in glycogen storage disease type Ia: a case series. J. Inherit. Metab. Dis. 2005;28:153–162. - PubMed
-
- Melis D., Cozzolino M., Minopoli G., Balivo F., Parini R., Rigoldi M., et al. Progression of renal damage in glycogen storage disease type I is associated to hyperlipidemia: a multicenter prospective Italian study. J. Pediatr. 2015;166:1079–1082. - PubMed
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
