

Influenza vaccine effectiveness in immunocompromised patients with cancer: A Danish nationwide register-based cohort study
- PMID: 39306693
- PMCID: PMC11694166
- DOI: 10.1002/cncr.35574
Influenza vaccine effectiveness in immunocompromised patients with cancer: A Danish nationwide register-based cohort study
Abstract
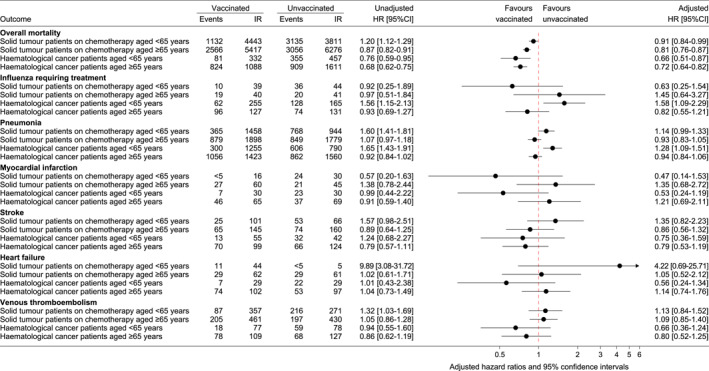
Background: Influenza vaccination is free of charge for Danish citizens with acquired immunodeficiency but recommendations do not specifically target patients with cancer. This study investigated whether influenza vaccination reduces the main outcome of overall mortality and the secondary outcomes of influenza requiring treatment, pneumonia, myocardial infarction, stroke, heart failure, and venous thromboembolism in patients with cancer.
Methods: This was a register-based nationwide cohort study. Adjusted hazard ratios (aHRs) and 95% confidence intervals (95% CIs) for overall mortality and secondary outcomes were estimated using Cox proportional hazards models. Analyses were conducted separately for four subgroups: patients aged <65 years with solid tumors, patients aged ≥65 years with solid tumors, patients aged <65 years with hematological cancer, and patients aged ≥65 years with hematological cancer.
Results: A total of 53,249 adult patients with solid tumors who received chemotherapy and 22,182 adult patients with hematological cancer were followed for up to five influenza seasons in the study period of 2007-2018. In the main analysis covering December-March, influenza vaccination was associated with reduced overall mortality in all four subgroups. The reduction was most pronounced in patients with hematological cancer aged <65 years (aHR, 0.66; 95% CI, 0.51-0.87) and smallest in patients with solid tumors aged <65 years (aHR, 0.91; 95% CI, 0.84-0.99). In sensitivity analyses covering January-March, the aHR was 0.87 (95% CI, 0.65-1.16) in patients with hematological cancer aged <65 years and 1.01 (95% CI, 0.92-1.10) in patients with solid tumors aged <65 years. Results for the secondary outcomes were inconclusive.
Conclusions: The results of this study cannot reject that influenza vaccination reduces overall mortality in immunocompromised patients with cancer. The results must be interpreted with caution because of potential unmeasured confounding, which can result in the overestimation of influenza vaccine effectiveness.
Keywords: chemotherapy; hematological cancer; immunosuppression; influenza vaccination; seasonal influenza; solid tumors.
© 2024 The Author(s). Cancer published by Wiley Periodicals LLC on behalf of American Cancer Society.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures




References
-
- Influenza (Seasonal). World Health Organization . Accessed June 28, 2024. https://www.who.int/news‐room/fact‐sheets/detail/influenza‐(seasonal)
-
- Warren‐Gash C, Blackburn R, Whitaker H, McMenamin J, Hayward AC. Laboratory‐confirmed respiratory infections as triggers for acute myocardial infarction and stroke: a self‐controlled case series analysis of national linked datasets from Scotland. Eur Respir J. 2018;51(3):1701794. doi: 10.1183/13993003.01794-2017 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
